Coronary OCT and CMR imaging to determine sex differences in underlying causes of myocardial infarction with no obstructive coronary arteries
Reported from ACC.26
Nicola Ryan provides her take on the trial evaluating multi-modality imaging to determine underlying causes of MINOCA in women and men. The trial results were presented by Harmony R. Reynolds at ACC.26 in New Orleans and simultaneously published in Circulation.
In patients with myocardial infarction with non-obstructive coronary arteries (MINOCA), this trial utilised three-vessel OCT and Cardiac MRI to evaluate the underlying cause, explore sex differences and identify predictors of imaging abnormalities.
Designed by Nicola Ryan. Source: PCRonline.com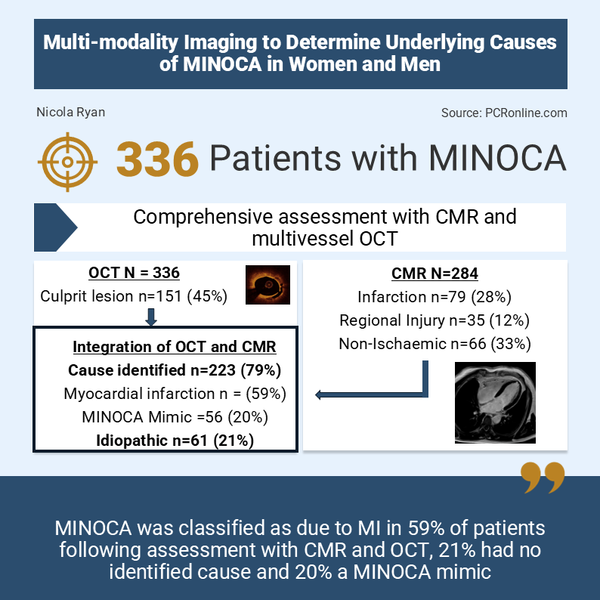
Why this study – the rationale/objective?
MINOCA is an umbrella term for patients who present with a clinical diagnosis of myocardial infarction with non-obstructive coronary arteries on coronary angiography. The underlying mechanisms for MINOCA are heterogenous and include unstable plaques (plaque rupture or erosion), coronary embolism, spontaneous coronary artery dissection and coronary vasospasm (epicardial or microvascular). An initial diagnosis of MINOCA may be superseded by a non-ischaemic mimicking condition such as takotsubo’s cardiomyopathy or myocarditis following full evaluation. Approximately 6-8% of patients presenting with an MI have MINOCA, which is associated with increased MACE therefore, identification and appropriate treatment of the underlying cause is of interest. Whilst MINOCA is more common in women than in men, it is encountered in both sexes.
How was it executed - the methodology?
The Heart Attack Research Programme was a prospective, observational multicentre diagnostic study applying standardised imaging protocols to patients with a clinical diagnosis of MINOCA. Initially, the study enrolled women only however, this was then expanded to include both sexes. Patients meeting the 4th universal definition of MI referred for coronary angiography were eligible for inclusion. Following diagnostic angiogram participations with no stenosis (≥50%) in a major epicardial vessel, the study protocol was OCT in all major epicardial arteries at the time of angiogram and CMR within one week of presentation.
OCT culprit lesions were assessed by a core lab and classified as plaque rupture, plaque erosion, intraplaque haemorrhage, healed plaque, calcified nodule or spontaneous coronary artery dissection. CMR was characterised as ischaemic or non-ischaemic, with the non-ischaemic further characterised as myocarditis, pericarditis, non-ischaemic cardiomyopathy with reduced LV systolic function, takotsubo cardiomyopathy, infiltrative cardiomyopathy or hypertrophic cardiomyopathy
- The primary objective was to determine the proportion of patients with vascular causes of MINOCA as identified by coronary OCT and the proportion of patients with CMR findings that could explain the clinical presentation.
- A secondary objective was to determine whether results of imaging differed by sex.
- MINOCA was classified as MI if CMR identified infarction or regional injury in a coronary territory or OCT identified a culprit lesion.
- A non-ischaemic cause was assigned if CMR demonstrated myocarditis, pericarditis, non-ischaemic cardiomyopathy, infiltrative disease, takotsubo syndrome, pulmonary embolism or hypertrophic cardiomyopathy with evidence of acute myocardial oedema.
- MINOCA was classified as idiopathic if no cause was identified using either imaging test.
What is the main result?
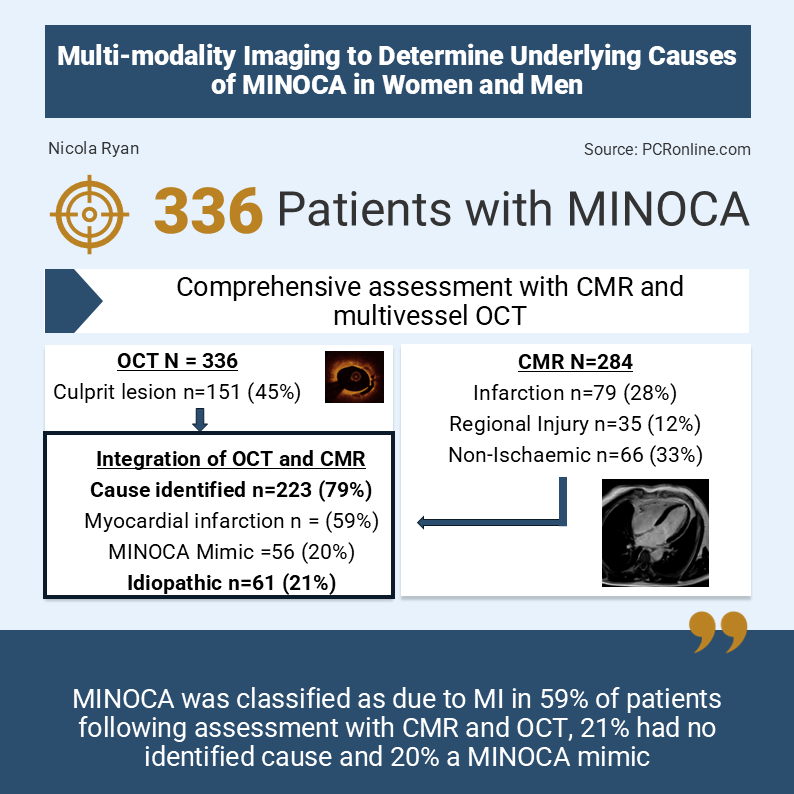
From 2016 to 2025, 754 patients, 539 women and 215 men were included in the study, of whom 389 had MINOCA, 317 women and 72 men. After exclusion of 53 patients with no OCT (48), missing OCT (2) or uninterpretable images (3), 336 patients were included in the study cohort. Of the OCT cohort, 64% had 3 vessel OCT, 29% 2 vessel OCT and 7% single vessel OCT. CMR was performed in 289 patients, with interpretable images in 284. (225 women, 59 men). The median time to CMR from diagnosis was 6 days (IQR 3-10). The mean age of the population was 58 years, with coronary angiography reported as normal by the treating site in 46%, 35% of patients had a regional wall motion abnormality on echocardiogram.
- OCT identified a culprit lesion in 45% (151/336) of patients with no differences between women (43%, 116/270) and men (53%, 35/66), p=0.141.
- Intraplaque haemorrhage (17%) was the most common culprit lesion, with layer plaque (12%), plaque rupture (7%) and plaque erosion (5%) seen commonly
- Eruptive calcified nodule (2%), thrombus without plaque (1%) and spontaneous coronary artery dissection were less frequently encountered.
- An ischaemic pattern of late gadolinium enhancement (LGE) was seen in 79 patients, 28% (28% of women 25% of men), with a regional injury (myocardial oedema in a single coronary territory) in an additional 35 patients, 12% (14% of women, 5% of men)
- Non-ischemic findings were identified in 66 patients
- Combined OCT and CMR identified a cause for MINOCA in 79% of patients, higher than OCT alone (124/284, 44%, 95%CI 38-49%, p<0.01) or CMR alone (180/284, 63%, 95%CI 58-69%, p<0.001)
- MI diagnosis 59%
- MINOCA mimic 20%
- Idiopathic MINOCA (no cause identified 21%)
Critical reading and the relevance for clinical practice
The results of this prospective observational study showed that a comprehensive diagnostic assessment with multivessel OCT and CMR in patients with MINOCA led to diagnosis of a mimicking condition in approximately 20% of the population. Amongst the remaining participants, 68% had imaging evidence of MI, an OCT-defined culprit lesion in 50%, CMR determined infarction in 52% with co-occurrence common. The information provided by OCT and CMR are complementary, as 41% of patients with a normal CMR had an OCT-defined coronary lesion, and 44% of patients with an MI identified by CMR did not have a culprit lesion identified on OCT.
Clinical characteristics were poor predictors of culprit lesions on OCT however, imaging all three vessels doubled the odds of identifying a culprit lesion. Older age and the severity of nonobstructive stenosis at angiography were predictors of a culprit lesion on OCT. Importantly, there were three complications, coronary dissections, associated with the use of intracoronary imaging, which led to PCI in these patients, one patient experiencing a small haemopericardium. Whilst OCT is generally safe it is important to weigh the benefit of OCT against the risk of coronary dissection particularly in tortuous arteries and ensure it is used judiciously.
An ischaemic pattern on CMR was more commonly seen in patients with culprit lesions on OCT (52% with vs 31% without culprit lesion p<0.001). However importantly ischaemia was seen in the absence of culprit lesions. There are a number of potential explanations for this, including absence of OCT in the territory of the ischaemia however, a transient embolic event should also be considered. An important limitation of the study is that provocation testing was not carried out. In the recent PROMISE (1) trial, epicardial spasm was found not uncommonly in the comprehensive assessment group, allowing appropriate risk stratification and medication optimisation. This would have been of particular interest in the group without a culprit lesion identified on OCT with evidence of ischaemia on CMR, as whilst epicardial spasm can cause plaque rupture and/or thrombus formation, the vasoconstriction alone can cause ischaemia.
When assessed by sex, there were no differences in the cause of MINOCA between men and women.
Some important limitations of the study include the absence of three-vessel OCT in all patients, which may lead to missed culprit lesions. Similarly, not all patients underwent CMR which is further hindered by the delay to CMR in patients. The diagnostic yield of CMR is highest when obtained within three days of the presentation, with decreased yield as the time from presentation increases. However, there is an important resource limitation with CMR with access to timely CMR not available in all healthcare systems/hospitals and similarly dedicated cardiac MRI machines are not always available when access to MRI is feasible.
Overall, this study adds to the evidence supporting the guideline recommendation of a comprehensive imaging assessment in patients with MINOCA to identify and treat the underlying cause. Further studies should focus on the integration of functional testing into the diagnostic/assessment algorithm to further refine the diagnosis. However despite a comprehensive diagnostic strategy in the PROMISE trial, 20% of patients remained undifferentiated beyond the original MINOCA diagnosis, similar to the numbers in this study. This highlights the ongoing need for investigations into the potential aetiologies of MINOCA. Ongoing training and education in intracoronary imaging acquisition and interpretation is required for the community at large.

No comments yet!