213 results
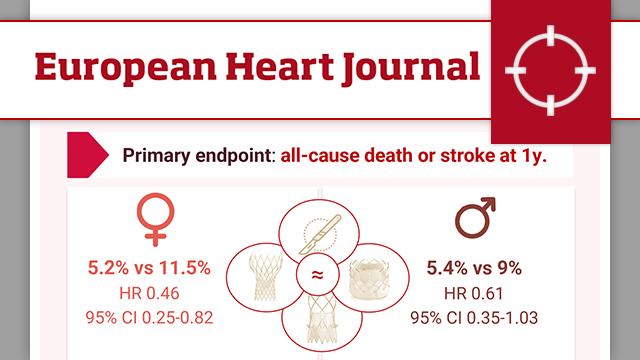
Sex-specific outcomes after transcatheter or surgical treatment of aortic valve stenosis: the DEDICATE-DZHK6 trial
30 Mar 2026
Women have long been underrepresented in TAVR trials. This article explores the DEDICATE trial’s sex-specific outcomes after TAVI and SAVR, revealing differences in early stroke risk, procedural challenges, and one-year survival in men and women with aortic stenosis.

Reviewer
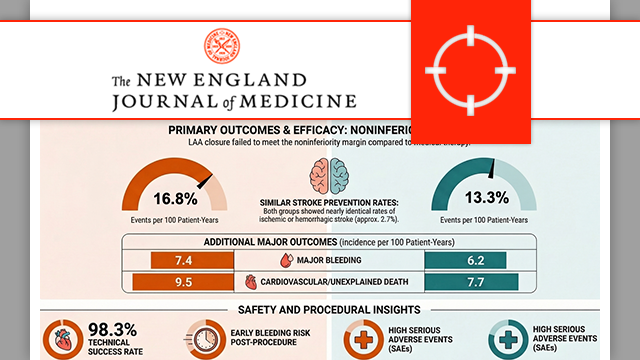
CLOSURE-AF: left atrial appendage closure or medical therapy in atrial fibrillation
23 Mar 2026
Catheter-based left atrial appendage closure (LAAC) is widely used as an alternative to oral anticoagulation in atrial fibrillation. But how does it compare with best medical therapy in patients at high risk of both stroke and bleeding? The CLOSURE-AF trial provides new data to inform this...

Reviewer
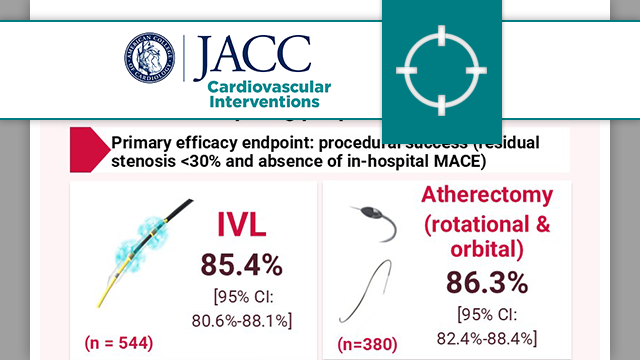
Intravascular lithotripsy or mechanical debulking in complex calcified coronary arteries: multicenter, prospective ROLLING STONE study
19 Mar 2026
The ROLLING STONE registry compares intravascular lithotripsy (IVL) and atherectomy (rotational and orbital) for treating heavily calcified coronary arteries, assessing real-world safety and effectiveness in percutaneous coronary interventions (PCI).

Reviewer
Bioresorbable vascular scaffold versus metallic drug-eluting stent in patients at high risk of restenosis: final 7-year results of the COMPARE-ABSORB trial
10 Mar 2026
This study provides the longest available follow-up for first-generation bioresorbable vascular scaffolds and fails to demonstrate any late clinical advantage after complete scaffold resorption.

Reviewer

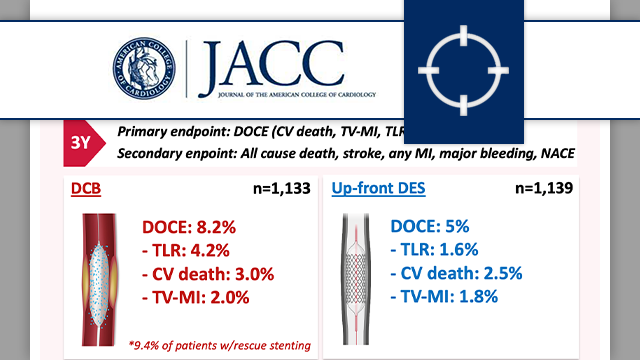
Drug-coated balloon angioplasty vs up-front stenting for de novo CAD: 3-year follow-up of REC-CAGEFREE I trial
10 Mar 2026
The 3-year follow-up of the REC-CAGEFREE I trial demonstrated that a DCB-based strategy with rescue stenting was associated with a significantly higher rate of DOCE compared with contemporary DES implantation in patients with de novo, non-complex coronary artery disease.

Reviewer

Reviewer
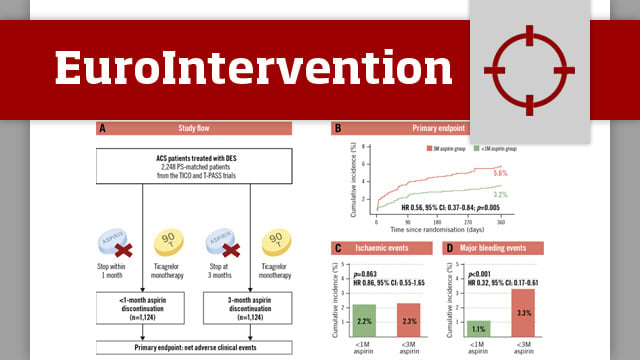
Aspirin discontinuation timing with ticagrelor monotherapy in ACS: a post hoc analysis from TICO and T-PASS
11 Mar 2026
The TICO1 and T-PASS2 trials evaluated abbreviated DAPT followed by ticagrelor monotherapy compared to DAPT in patients with ACS undergoing PCI. Both trials demonstrated the safety and efficacy of abbreviated DAPT however, the optimal timing of aspirin discontinuation remains uncertain. This post hoc analysis compares the...

Reviewer
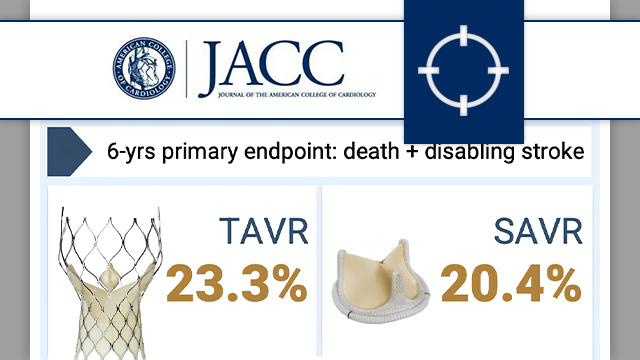
Six-year outcomes after transcatheter vs surgical aortic valve replacement in low-risk patients with aortic stenosis
25 Feb 2026
The 6-year results of the Evolut Low Risk trial confirm the absence of significant differences in the composite primary endpoint between TAVR and surgery, but introduce an important nuance: the first signal of increased valve reintervention in the TAVR arm within this trial.

Reviewer
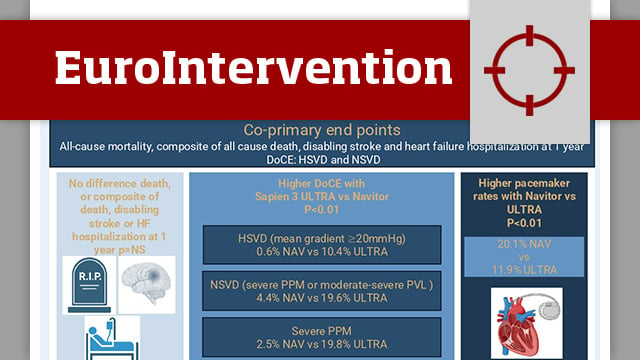
Intra-annular self-expanding or balloon-expandable TAVI in small annuli: the NAVULTRA registry
17 Feb 2026
Patients with severe symptomatic aortic stenosis and small annuli—most often women—face higher risks of elevated gradients, patient–prosthesis mismatch and early valve failure after TAVI, with added challenges for future coronary access and redo procedures, particularly in younger populations.
While previous studies have mainly compared supra-annular balloon- and...

Reviewer
Ticagrelor vs prasugrel in patients with diabetes and multivessel coronary artery disease: the TUXEDO-2 randomised clinical trial
17 Feb 2026
The TUXEDO-2 trial sought to directly compare prasugrel versus ticagrelor in diabetic patients undergoing percutaneous coronary intervention (PCI), with the aim of clarifying whether the non-inferiority of ticagrelor could be established.

Reviewer
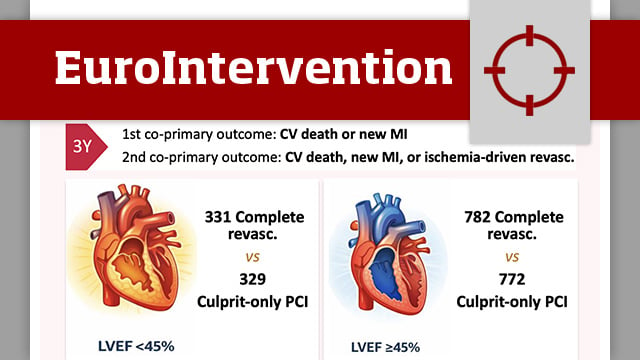
Impact of complete revascularisation in relation to left ventricular function in patients with ST-segment elevation myocardial infarction and multivessel disease: a post hoc analysis of the COMPLETE randomised trial
05 Feb 2026
This study represents a prespecified subgroup analysis of the COMPLETE randomised trial, a large, international, randomised controlled study comparing a strategy of complete revascularisation with culprit-only percutaneous coronary intervention (PCI) in patients presenting with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease (MVD).
The present...
Reviewer
Reviewer