Geographical variations in left main coronary artery revascularisation: a prespecified analysis of the EXCEL trial
Selected in EuroIntervention Journal by M. Alasnag , A. Al Saleh
The purpose of the prespecified subanalysis of the EXCEL (Evaluation of XIENCE versus Coronary artery bypass surgery for Effectiveness of Left main revascularization) trial was to determine whether the outcomes remained consistent regardless of geography.
References
Authors
Aung Myat, David Hildick-Smith, Adam J. de Belder, Uday Trivedi, Aaron Crowley, Marie-Claude Morice, David E. Kandzari, Nicholas J. Lembo, W. Morris Brown III, Patrick W. Serruys, Arie Pieter Kappetein, Joseph F. Sabik III, Gregg Stone
Reference
EuroIntervention 2022;17:1081-1090. DOI: 10.4244/EIJ-D-21-00338
Published
January, 28 2022
Link
Read the abstract
Reviewers


Our Comment
Why this study – the rationale/objective?
The Evaluation of XIENCE versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization (EXCEL) trial was a prospective, open-label, multicenter, international study of 1,900 randomised patients with significant Left Main disease (LM) stenosis.
Patients were randomised 1:1 to undergo percutaneous coronary intervention (PCI) using cobalt-chromium everolimus-eluting stents (CoCr-EES) or coronary artery bypass grafting (CABG).
The five-year results of the primary endpoint (a composite rate of death, stroke, or myocardial infarction (MI)) reported no significant difference between PCI and CABG in those with a SYNTAX score ≤ 321.
The 30-day adverse events of PCI in the EXCEL trial were lower than CABG. The trial was conducted between 2010 and 2014.
In the main trial design, investigators noted that the EXCEL trial had sufficient geographic representation and power to establish the roles of CABG and PCI. As such, the purpose of the prespecified subanalysis of the EXCEL trial by Myat et al was to determine whether the outcomes remained consistent regardless of geography2.
It is important to understand the impact of geographic variations in patient demographics, operator expertise, and techniques, available pharmacotherapies, and uptake of intracoronary imaging (IVUS).
There were 126 centers from 17 countries including Europe, USA, Canada, South America, Asia, and Australia involved in this study.
How was it executed? - the methodology
Randomisation was stratified according to the recruiting site. In addition, site-assessed SYNTAX score and site-determined procedural strategies including IVUS use and site-determined number and type of bypass conduits were part of the protocol.
The primary endpoint was the composite of all-cause mortality, MI, or stroke at three years.
Secondary endpoints included the composite endpoint at 30 days, and the composite of death, MI, stroke, or ischaemia-driven revascularisation at 3 years.
Clinical follow-up was performed at 1 month, 6 months, 1 year, and annually up to five years.
Interaction testing was performed to determine whether the relative risk of the major outcome measures at 30 days, 3 years, and 5 years after PCI versus CABG varied by geographic location. Results for an intention-to-treat analysis were reported.
What is the main result?
The study randomized 948 to PCI and 957 to CABG.
Fifty-six percent (1,075) were enrolled at 52 European countries and 39.5 % (795) were in North America (NA). Only 4.1 % from other international sites including Argentina, Brazil, South Korea, and Australia.
The baseline demographics and angiographic findings of both comparator arms were balanced when evaluated by region.
The NA cohort had more risk factors such as diabetes, obesity, and hypertension. The NA sites recruited more women and those with a prior PCI. The European cohort had a higher mean SYNTAX score and more distal LM bifurcation disease. Both cohorts were relatively young, with an average age of 66 years, preserved left ventricular function with an average ejection fraction of 57 % and < 2 % had an ST elevation MI.
In spite of more complex anatomy, the European cohort was less likely to have fewer treated lesions and stents used, less frequent post dilatation, less use of hemodynamic support, and longer time to randomization. They also used radial access more frequently. Interestingly, use of IVUS and fractional flow reserve was marginally higher in NA than in Europe although not statistically significant.
Both in NA and European centers, a provisional strategy was adopted more commonly than an upfront 2-stent strategy. In terms of CABG, it was more likely to be off-pump with all arterial grafts (although fewer vessels were bypassed. The European cohort had a longer hospital stay irrespective of the revascularization strategy.
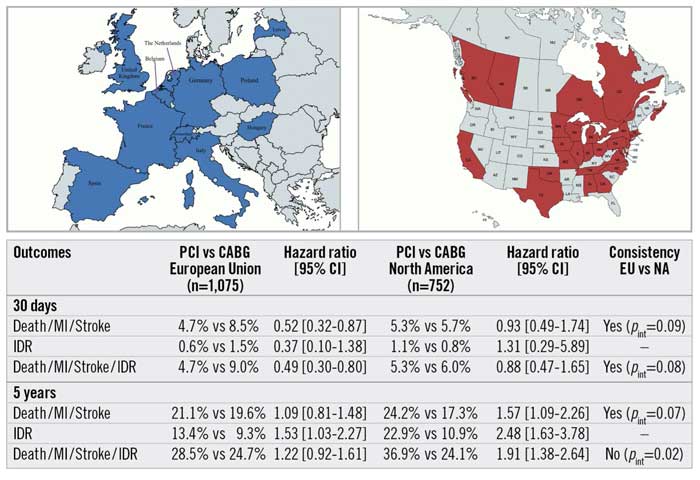
The 30-day outcomes were similar in the NA and European populations; ie the composite of death, MI, or stroke occurred less frequently after PCI compared with CABG, driven by a lower rate of MI. All-cause death was, however, higher in the European population. At 3 and 5 years, death rates were similar, but the ischemia-driven revascularization was higher in the North American group.
Other territories were not adequately studied given the smaller number of enrolled patients. What is notable is that the Asian populations tended to have higher rates of diabetes and smoking. Unlike a recent metanalysis noting better outcomes with CABG in women in Western population, this was not identified in Asian cohorts3. Considerable variation was also noted in the pharmacological treatment.
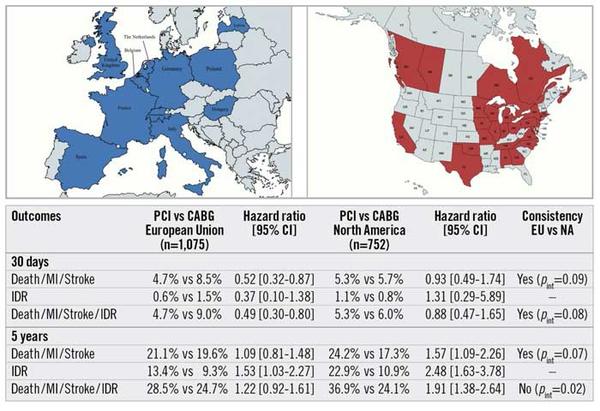
Geographical variations in left main coronary artery revascularisation outcomes from the EXCEL trial.
CABG: coronary artery bypass graft; CI: confidence interval; EU: European Union; IDR: ischaemia-driven revascularisation; MI: myocardial infarction; NA: North America; PCI: percutaneous coronary intervention; pint: p-value for interaction
Source: EuroIntervention Journal
Critical reading and the relevance for clinical practice
We often discuss results of large landmark clinical trials in terms of the details: “the devil is in the details”.
In this particular analysis, do we need the details if the broader primary and secondary endpoints remain consistent? In spite of the higher rate of ischemia driven revascularization in the NA cohort and the higher all-cause death at 30 days in the European cohort, the long-term outcomes of those with an intermediate or low Syntax Score remain similar irrespective of the region, suggesting that the decision should be individualized, and patient-centered.
However, the results cannot be extended to low volume operators or territories outside the NA and Europe, particularly regions with a high incidence of diabetes and diffuse disease.
Furthermore, these are all patients who have been pre-selected and their anatomy deemed amenable to either surgical or percutaneous revascularization.
Finally, although the enrollment ended in 2014, IVUS use was high (74 % European group and 80 % NA group). Additionally, in line with the recent EBC Main trial, a provisional strategy was employed more commonly in both studied regions (67 % European group & 61 % NA group)4. Whether a 2-stent strategy led to a higher rate of ischemia-driven revascularization or worse outcomes especially in other regions cannot be ascertained from this study.
References
- Stone GW, Kappetein AP, Sabik JF, Pocock SJ, Morice MC, Puskas J, Kandzari DE, Karmpaliotis D, Brown WM 3rd, Lembo NJ, Banning A, Merkely B, Horkay F, Boonstra PW, van Boven AJ, Ungi I, Bogáts G, Mansour S, Noiseux N, Sabaté M, Pomar J, Hickey M, Gershlick A, Buszman PE, Bochenek A, Schampaert E, Pagé P, Modolo R, Gregson J, Simonton CA, Mehran R, Kosmidou I, Généreux P, Crowley A, Dressler O, Serruys PW; EXCEL Trial Investigators. Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease. N Engl J Med. 2019 Nov 7;381(19):1820-1830. doi: 10.1056/NEJMoa1909406. Epub 2019 Sep 28. Erratum in: N Engl J Med. 2020 Mar 12;382(11):1078.
- Myat A, Hildick-Smith D, de Belder AJ, Trivedi U, Crowley A, Morice MC, Kandzari DE, Lembo NJ, Brown WM III, Serruys PW, Kappetein AP, Sabik JF III, Stone G. Geographical variations in left main coronary artery revascularisation: a prespecified analysis of the EXCEL trial. EuroIntervention. 2022 Jan 28;17(13):1081-1090. doi: 10.4244/EIJ-D-21-00338.
- Sotomi Y, Onuma Y, Cavalcante R, Ahn JM, Lee CW, van Klaveren D, de Winter RJ, Wykrzykowska JJ, Farooq V, Morice MC, Steyerberg EW, Park SJ, Serruys PW. Geographical Difference of the Interaction of Sex With Treatment Strategy in Patients With Multivessel Disease and Left Main Disease: A Meta-Analysis From SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery), PRECOMBAT (Bypass Surgery Versus Angioplasty Using Sirolimus-Eluting Stent in Patients With Left Main Coronary Artery Disease), and BEST (Bypass Surgery and Everolimus-Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) Randomized Controlled Trials. Circ Cardiovasc Interv. 2017 May;10(5):e005027. doi: 10.1161/CIRCINTERVENTIONS.117.005027.
- Hildick-Smith D, Egred M, Banning A, Brunel P, Ferenc M, Hovasse T, Wlodarczak A, Pan M, Schmitz T, Silvestri M, Erglis A, Kretov E, Lassen JF, Chieffo A, Lefèvre T, Burzotta F, Cockburn J, Darremont O, Stankovic G, Morice MC, Louvard Y. The European bifurcation club Left Main Coronary Stent study: a randomized comparison of stepwise provisional vs. systematic dual stenting strategies (EBC MAIN). Eur Heart J. 2021 Oct 1;42(37):3829-3839. doi: 10.1093/eurheartj/ehab283.
No comments yet!