19 Mar 2026
Intravascular lithotripsy or mechanical debulking in complex calcified coronary arteries: multicenter, prospective ROLLING STONE study
Selected in JACC: Cardiovascular Interventions by A. Cader
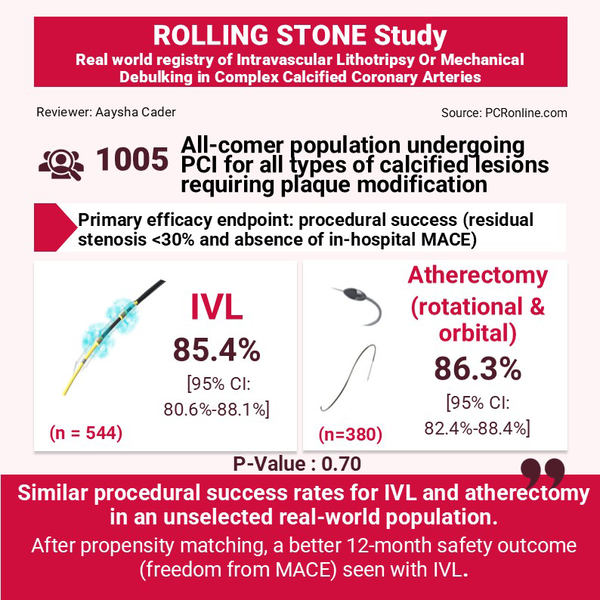
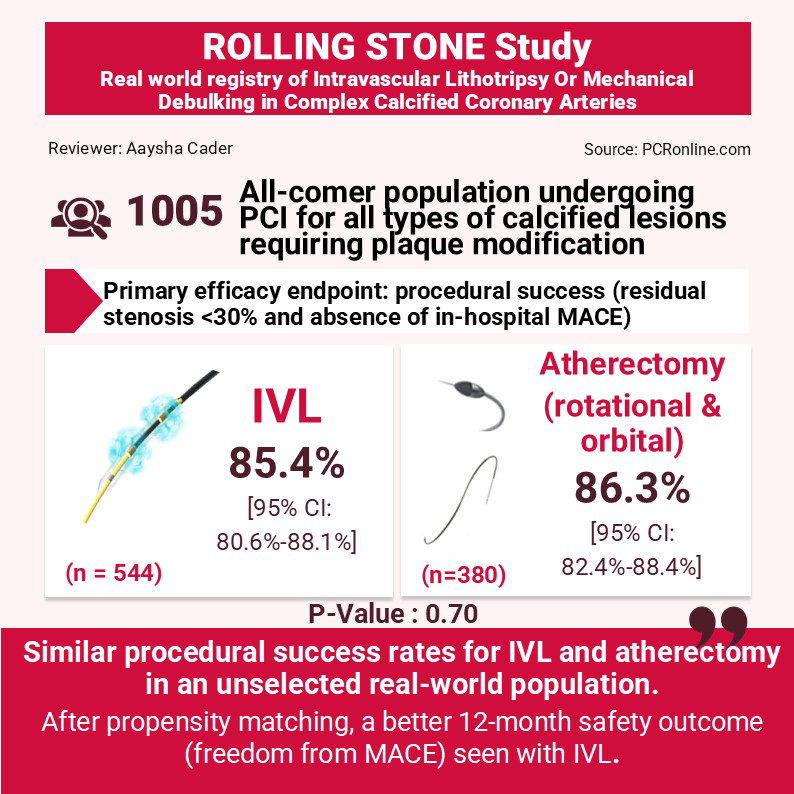
The ROLLING STONE registry compares intravascular lithotripsy (IVL) and atherectomy (rotational and orbital) for treating heavily calcified coronary arteries, assessing real-world safety and effectiveness in percutaneous coronary interventions (PCI).
References
Authors
Enrico Cerrato, Marco Pavani, Simone Zecchino, Massimo Leoncini, Greca Zanda, Mohamed Abdirashid, Stefano Cordone, Annamaria Nicolino, Alfonso Franzè, Alessandro Bernardi, Veronica Lio, Alberto Boi, Giorgio Marengo, Davide Giacomo Presutti, Paolo Vadalà, Gioel Gabrio Secco, Federico Conrotto, Rocco Vergallo, Alberto Menozzi, Paola Berchialla, Francesco Tomassini, Giuseppe Patti, Giuseppe Musumeci, Alessandra Chinaglia, and Ferdinando Varbella
Reference
JACC: Cardiovascular Interventions Volume 19, Number 5
Published
29 January 2026
Link
Read the abstractReviewer

My Comment
Key insights from the ROLLING STONE study, summarised in this infographic by A. Cader.
Why this study – the rationale/objective?
Percutaneous coronary interventions (PCI) for heavily coronary artery calcifications are associated with technical difficulty (stent delivery, suboptimal stent expansion), lower procedural success and higher rates of adverse events.
The ROLLING STONE registry aimed to compare the effectiveness and safety of (i) intravascular lithotripsy (IVL) vs (ii) Atherectomy (AT) – i.e. rotational atherectomy (RA) and orbital atherectomy (OA) in a real-world, all-comer population1.
How was it executed? The methodology
This was a prospective, multicentre, open-label, investigator-initiated all-comers registry conducted across 23 hospitals in Italy.
Study population:
All patients undergoing PCI for calcified coronary artery disease requiring plaque modification using AT (RA by ROTAPRO system; OA by Diamondback 360 Coronary orbital atherectomy system) or/and IVL (Shockwave lithotripsy) were included.
All types of calcified lesions were eligible, including de novo lesions, calcified in stent restenosis (ISR), and acute coronary syndromes (ACS). Severely calcified lesions were based on angiographic selection by operator. Patients were enrolled before starting 1 of the selected debulking techniques. Procedural strategy including lesion preparation and use 0f intravascular imaging was left to operator discretion.
Endpoints:
The primary effectiveness endpoint was procedural success, defined as residual stenosis < 30 % (core lab assessed) and absence of intraprocedural major adverse cardiac events (MACE) (cardiac death, myocardial infarction [MI], or target vessel revascularisation).
The primary safety endpoint was freedom from MACE within 30 days of the index procedure.
Statistical analysis included comparison of IVL vs AT devices (RA, and OA). Propensity score matching (PSM) and inverse probability weighting (IPW) were performed to compare 30-day and 12-month safety endpoints in the 2 groups.
What is the main result?
A total of 1,005 consecutive patients requiring PCI for calcified lesions in whom a calcium debulking was deemed necessary were enrolled, from January 10, 2022, to December 31, 2023. 544 were in the IVL group, and 380 in the AT group were analysed. 81 patients (8 %) were excluded, in whom both IVL and an AT device (RA or OA) at the same target lesion were used.
Baseline clinical characteristics differed significantly, this being a non-randomised, all-comer cohort. Those in the IVL group subjects were slightly younger (median 75 years vs 76 years ; P = 0.031). The majority (56 %) of patients presented with ACS.
Procedural characteristics:
Almost 80 % of cases presented multivessel disease. IVL was used in 80 % (435/544) of cases for de novo lesions, 11 % for in-stent restenosis, and 10 % of cases as a bailout strategy for acute stent under expansion; a second balloon was required in 5 % cases. Conversely, AT was exclusively used for de novo lesions. A second burr was needed in 14 % of RA procedures; in one-half of OA cases, both low- and high-speed settings were employed.
Radial access was more frequently used in IVL (85 %) than in the AT group (74 %) (P = 0.001).
Intravascular imaging was also more commonly used with IVL than AT (38 % vs 28 % ; P = 0.003). Atherectomy patients had a higher prevalence of multivessel disease (84 % vs 74 % ;P < 0.001) and longer stented segments, than IVL.
Outcomes:
Procedural success rates were similar between groups (in IVL 85.4 % [95 % CI: 80.6 %-88.1 %]; in AT 86.3 % [95 % CI: 82.4 %-88.4 %]; P = 0.70). Intraprocedural complications were similar, although AT was associated with more access site complications (2.5 % vs 0.7 %; P = 0.03). In-hospital MACE rate was 4.4 % in the IVL group compared with 7.3 % in the AT group (RR: 0.62; 95 % CI: 0.36-1.08).
MACE rate at 30 days was significantly lower in the IVL group (5.7 % vs 8.6 %; HR: 0.60; 95 % CI: 0.36-0.99; P = 0.045), driven primarily by a lower rate of cardiovascular death (1.7 % vs 3.9 %; HR: 0.40; 95 % CI: 0.18-0.92; P = 0.030). No significant differences were observed at 12 months (11 % vs 14 %; HR: 0.71; 95 % CI: 0.49-1.04; P = 0.079). However, after propensity score matching (n = 320) and inverse probability weighting (n = 532), the MACE rate at 12 months was significantly lower in the IVL group (6.8 % vs 14.3 %; HR: 0.43; 95 % CI: 0.21-0.89; P = 0.022).
Critical reading and the relevance for clinical practice:
ROLLING STONE is the largest prospective, investigator-initiated, multicentre registry and provides contemporary data on trends, outcomes and feasibility of calcium modification strategies in a real-world population. Given 56 % of the cohort presented with ACS, the study indicates the safety of using calcium debulking in these high-risk populations who might be more prone to slow-flow/no reflow.
The study was, however, observational, and the data must be interpreted in the context of some limitations. Firstly, the inclusion criterion for severe calcification was left to operator discretion, likely involved angiographic determination and was not clearly defined by core-lab analysed intravascular imaging criteria, rendering some selection bias. Indeed, imaging was used in less than a third of cases overall, which may reflect real-world practice, but may have influenced procedural success. Angiograms were however analysed by a blinded core lab and outcomes were adjudicated by an independent events committee.
Device selection may also have been prone to bias, given operator discretion, which may have been influenced by individual comfort levels with the device as well as complexity of the lesions, thus the performance of one device against another was not strictly assessed in the same degree of calcification or complexity. Comparisons were made of IVL against both atherectomy strategies in combination, thus nuanced indications specific for RA or OA were not captured. Furthermore, patients in whom a hybrid strategy was used, were excluded, constituting 8 % of the cohort, reflecting real-world practice wherein combinations of debulking tools may need to be used to optimise results.
Finally, reasons for temporal differences in outcomes, wherein similar in-hospital MACE rates but worse outcomes for OA at 30 days and 12 months (by PSM) were observed, have not been clearly explained.
Reference
- Cerrato E, Pavani M, Zecchino S, Leoncini M, Zanda G, Abdirashid M, et al. Intravascular Lithotripsy or Mechanical Debulking in Complex Calcified Coronary Arteries: Multicenter, Prospective ROLLING STONE Study. JACC Cardiovasc Interv. 2026 Mar 9;19(5):571-582. doi: 10.1016/j.jcin.2025.11.033. Epub 2026 Jan 29. PMID: 41609534.

