Coronary microvascular dysfunction and cardiovascular outcomes: FLOW-CMD Registry
Selected in The Lancet by R. Piccolo , A. Scibelli
Coronary microvascular dysfunction is increasingly recognised as a key determinant of outcomes beyond epicardial coronary disease. The FLOW-CMD registry provides new insights into its prevalence and prognostic impact in routine invasive practice.
References
Authors
Assoc Prof Joo Myung Lee, Seung Hun Lee, Dong Hyun Gim, Sang Yoon Lee, Ki Hong Choi, Joon Ho Ahn, Prof Young Joon Hong, Prof Hyun Kuk Kim, Kwan Yong Lee, Eun Ho Choo, Ki-Hyun Jeon, Hangyul Kim, Min Gyu Kang, Prof Jin-Sin Koh, Hyun Sung Joh, Taek Kyu Park, Prof Jeong Hoon Yang, Prof Young Bin Song, Prof Seung-Hyuk Choi, Prof Hyeon-Cheol Gwon, Prof Joo-Yong Hahn, for the Multicenter FLOW-CMD investigators
Reference
DOI: 10.1016/S0140-6736(26)00666-5 - Volume 407, Issue 10545 p 2319-2328 June 06, 2026
Published
June 06, 2026
Link
Read the abstractReviewers


Our Comment
Main results of the FLOW CMD Registry
Why this study – the rationale/objective?
Ischaemic heart disease has been traditionally associated with the evaluation and treatment of epicardial coronary arteries. However, conductive epicardial coronary arteries represent only 5-10% of coronary circulation, meanwhile arterioles and capillaries cover the remaining 90-95%.
Over the past two decades, it has been increasingly recognised that coronary microvascular disfunction is a major cause of ischaemic heart disease irrespective of epicardial coronary artery disease. Nevertheless, in routine clinical practice, the impact of microvascular disease is predominantly evaluated in patients with angina symptoms and clinical evidence of ischaemic heart disease, but absence of obstructive coronary artery atherosclerosis, considering the two entities as distinct.
The multicentre FLOW-CMD registry has tried to overcome these limits by prospectively evaluating the prevalence and prognosis of coronary microvascular disease in patients undergoing invasive coronary angiography in routine practice, irrespective of epicardial coronary artery disease.
How was it executed? The methodology
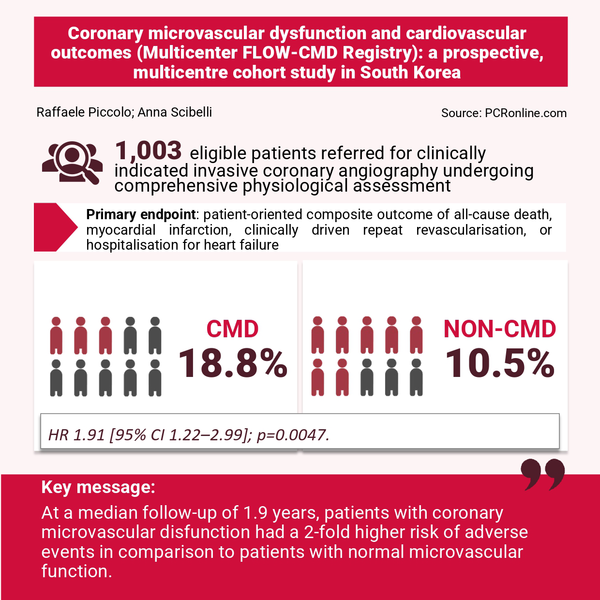
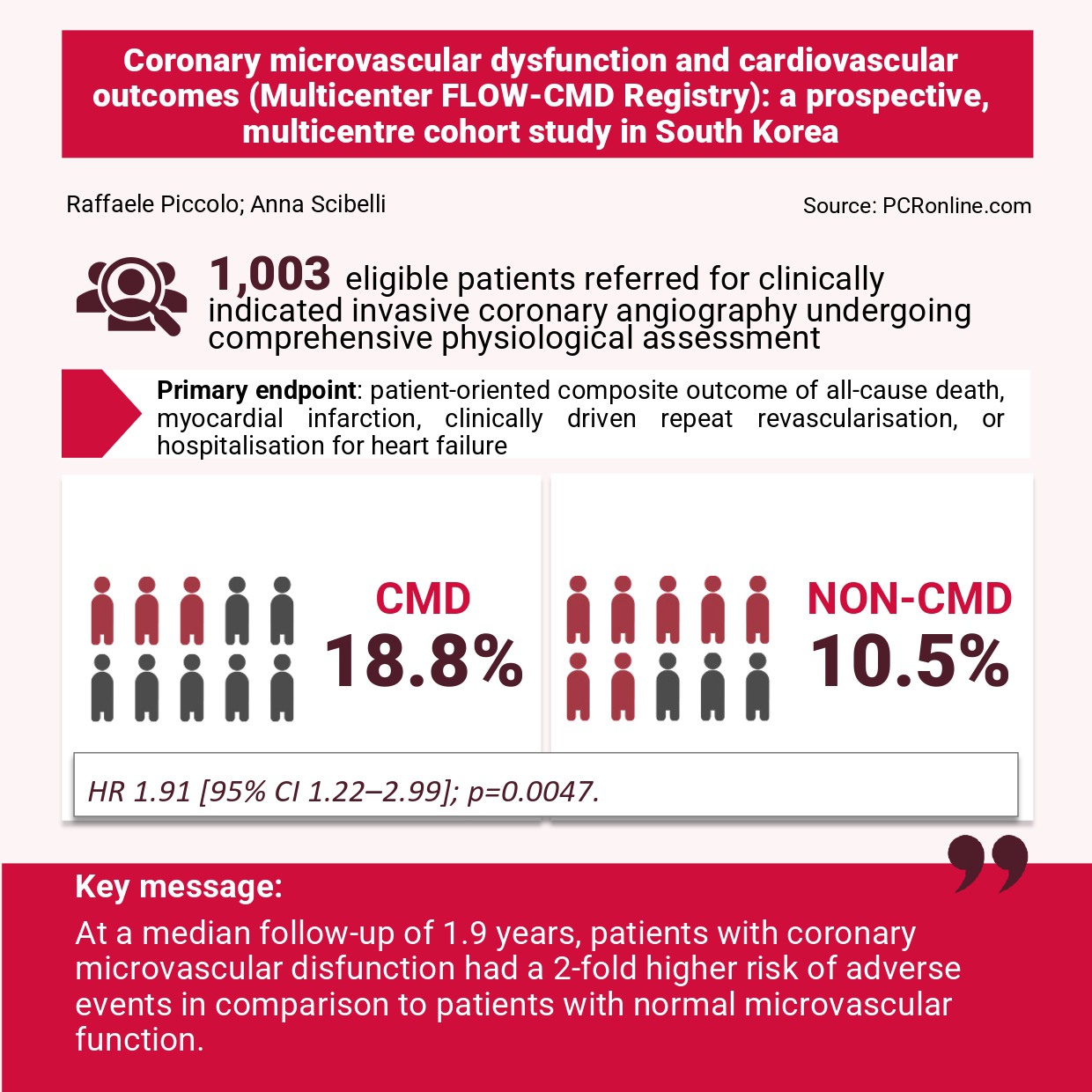
FLOW-CMD Registry is an investigator-initiated, prospective, multicentre cohort study. A total of 5,764 patients, who were referred for clinically indicated invasive coronary angiography, were screened; among these, all participants with intermediate epicardial stenosis underwent comprehensive physiological assessment, including FFR, CFR, and IMR. Eligible patients were enrolled if all three physiological indices had been obtained in at least one coronary artery.
- Obstructive epicardial coronary artery disease was defined as an intermediate stenosis (40–90% diameter stenosis) with FFR of 0.80 or less or severe stenosis (> 90%) treated with revascularisation without FFR measurement. Coronary microvascular dysfunction was identified as CFR lower than 2.0 and IMR of ≥ 25;
- The primary endpoint was a patient-oriented composite outcome of all-cause death, myocardial infarction, clinically driven repeat revascularisation, or hospitalisation for heart failure.
What is the main result?
A total of 1,003 patients were enrolled: 339 (33.8%) presented with ACS and 162 (16.2%) had no angiographically significant stenosis.
- Among the 1,003 patients, 163 (16.3%) had microvascular dysfunction, whereas 840 patients (83.7%) had preserved microvascular function. When stratified by the presence of obstructive epicardial stenosis, coronary microvascular dysfunction was observed in 123 (21.5%) of 573 patients with obstructive epicardial coronary artery disease and in 40 (9.3%) of 430 patients without obstructive epicardial coronary artery disease.
- At a median follow-up of 1.9 years, patients with coronary microvascular disfunction had a 1.91 times higher risk of reaching the primary endpoint than patients with normal microvascular function (95% confidence interval [CI] 1.22-2.99, p = 0.0047). In particular, 26 patients out of 163 with microvascular disfunction experienced the outcome, with an estimated 2-year event rate of 18.8%. Conversely, among the 840 patients with preserved microvascular function, only 70 experienced the primary endpoint, with an estimated 2-year event rate of 10.5%.
- Importantly, subgroup analysis showed that coronary microvascular dysfunction among patients without obstructive epicardial coronary artery disease was associated with a 3.5-fold higher risk of the primary endpoint compared with preserved microvascular function (HR 3.45, 95% CI 1.69–7.06; p = 0.0003).
- In addition, there was heterogeneity in the between the risk associated with CMD and the treatment strategy. Specifically, in the subset of patients undergoing PCI, CMD was not associated with a higher risk of the primary outcome (HR 1.31, 95% CI 0.70-2.45). In patients treated medically, CMD was associated with an increased risk of the primary outcome (HR 3.48, 95% CI 1.81-6.67, P for interaction = 0.034).
Critical reading and the relevance for clinical practice
The multicenter FLOW-CMD Registry addressed the clinically important question of whether microvascular dysfunction should be evaluated among patients undergoing invasive angiography.
Current guidelines primarily recommend the evaluation of coronary microvascular dysfunction within the diagnostic framework of ANOCA/INOCA, according to its established association not only with angina symptoms but also with adverse cardiovascular outcomes. Consistent with these observations, the present registry demonstrated a higher incidence of the primary endpoint among patients with coronary microvascular dysfunction compared with those with preserved microvascular function, supporting the prognostic relevance of microvascular impairment beyond its role in symptom generation.
Nevertheless, an important finding was that the prevalence of coronary microvascular dysfunction was higher among patients with concomitant obstructive epicardial coronary artery disease. Furthermore, the incidence of the primary endpoint was significantly greater in patients with coronary microvascular dysfunction, both among those with angiographically normal coronary arteries and in the overall study population. The multivariable analysis confirmed the role of coronary microvascular dysfunction as an independent risk factor of the primary endpoint.
The analysis of the individual components of the primary endpoint showed a higher incidence of repeat revascularisation in patients with vs without (8.8% vs 4%), with a heightened risk of non-target vessel revascularisation (4.6% vs 1%).
A plausible explanation of this evidence may be the impact of coronary microvascular dysfunction on the endothelial dysfunction and inflammatory pathways, and its role in atherosclerotic progression. Another potential explanation may be that the higher rate of angina after PCI observed in patients with coronary microvascular dysfunction may have led to the repetition of coronary angiography, resulting in the treatment of lesions that were not haemodynamically significant at baseline but subsequently progressed over time.
The results further suggested a significantly higher incidence of cardiovascular death among patients with CMD compared with those with preserved microvascular function. Notably, this risk excess was not accompanied by a corresponding increase in the incidence of myocardial infarction. Evaluation of the causes of death suggests a predominance of heart failure-related deaths rather than ischemia-related events. These findings, which deserve further investigation, may suggest that CMD patients may require more careful surveillance of heart failure. This hypothesis is in part supported by higher NT-proBNP levels among patients with CMD in comparison to those with preserved microvascular function.
Of interest, recent evidence has highlighted a high prevalence of CMD among patients with heart failure, including both reduced and preserved ejection fraction. Further investigations are needed to clarify the interplay between these two entities and to determine the extent to which each may influence the development, progression, and prognosis of the other.
No comments yet!