Quantitative flow ratio versus fractional flow reserve: 2-year follow-up of the FAVOR III Europe trial
Selected in EuroIntervention Journal by M. Gökalp , A. Nazmi Calik
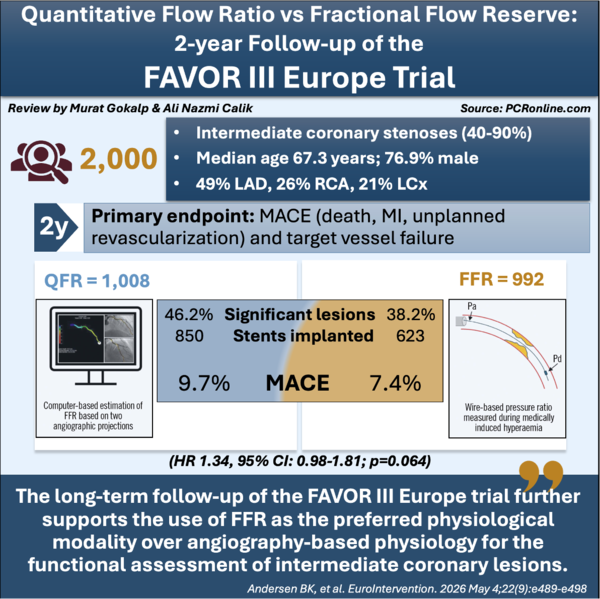
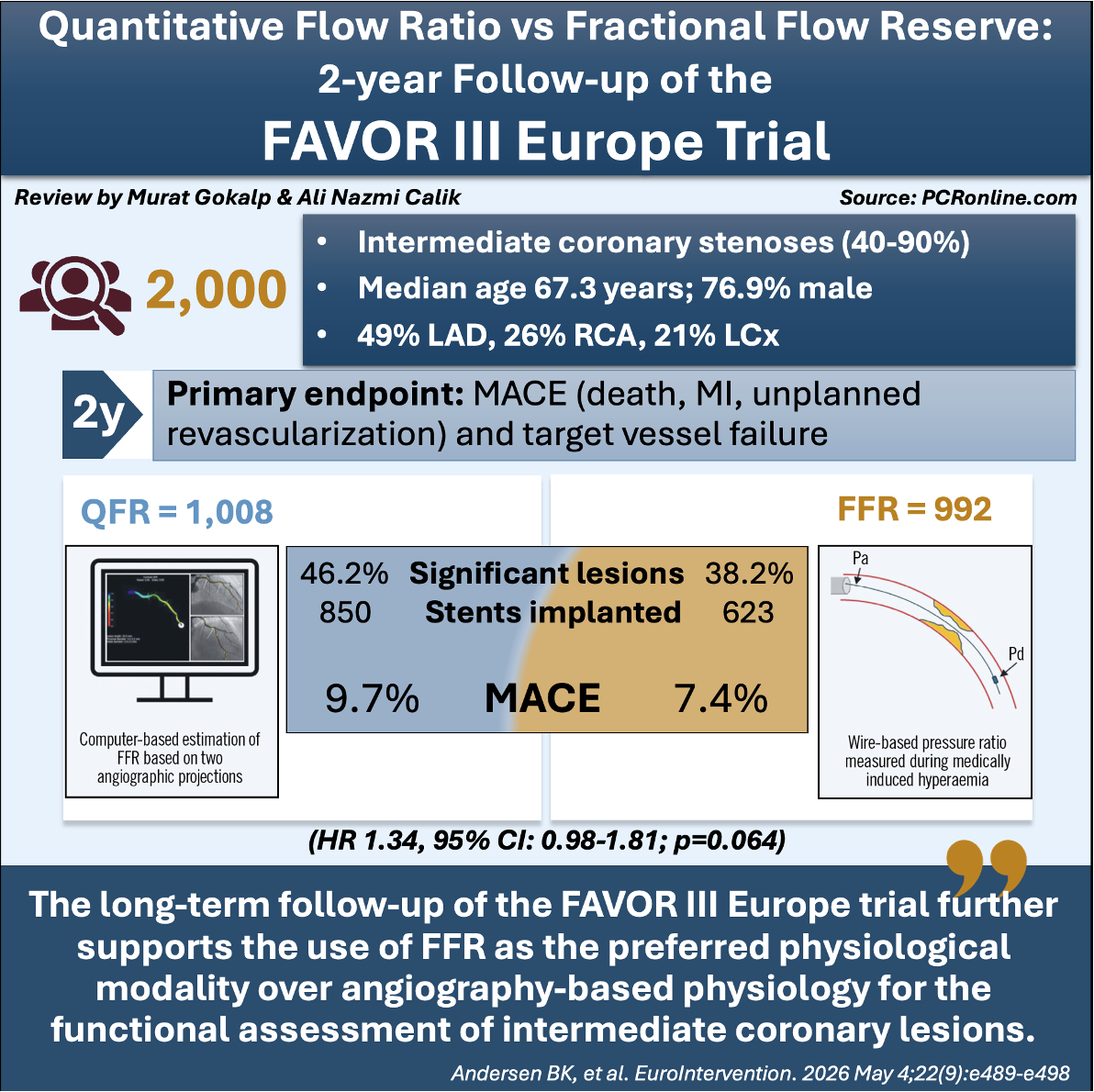
This study reports the prespecified 2-year follow-up results of the FAVOR III Europe trial, which compared quantitative flow ratio (QFR)-guided versus fractional flow reserve (FFR)-guided coronary revascularisation in patients with angiographically intermediate coronary stenoses.
FAVOR III Europe was a prospective, multicentre, randomised trial designed to evaluate whether an angiography-derived physiological assessment strategy could provide clinical outcomes comparable to those achieved with the current invasive reference standard, FFR. A total of 2,000 patients from 34 European centres were randomly assigned to QFR-guided or FFR-guided revascularisation and were followed for clinical outcomes over 2 years.
References
Authors
Birgitte K. Andersen; Niels R. Holm; Martin Sejr-Hansen; Andrea Erriquez; Truls Råmunddal; Barbara E. Stähli; Vincenzo Guiducci; Lone J.H. Mogensen; Jelmer Westra; Javier Escaned; Evald H. Christiansen; on behalf of the FAVOR III Europe investigators
Reference
DOI: 10.4244/EIJ-D-25-01255
Published
May 4, 2026
Link
Read the abstractReviewers


Our Comment
Infographic: key findings from the 2-year follow-up of the FAVOR III Europe trial
Why this study – the rationale/objective?
Physiology-guided revascularisation is recommended for the assessment of intermediate coronary stenoses, with fractional flow reserve (FFR) remaining the reference standard for functional lesion evaluation1. However, the need for pressure wires, hyperaemic agents, additional procedural time, and increased costs has limited its widespread adoption in routine clinical practice2.
Quantitative flow ratio (QFR) is an angiography-based physiological assessment method that estimates lesion significance without the need for pressure wires or pharmacologically induced hyperaemia. Previous validation studies demonstrated good agreement between QFR and FFR, while the FAVOR III China trial showed improved clinical outcomes with QFR-guided PCI compared with angiography-guided revascularisation3,4. Together, these findings contributed to the incorporation of angiography-derived physiology into contemporary European guidelines.
Despite these encouraging data, QFR had not been directly compared with FFR in a large randomised trial powered for clinical outcomes. The 1-year results of the FAVOR III Europe trial challenged the existing evidence by demonstrating that QFR failed to meet the criterion for non-inferiority to FFR and was associated with higher rates of revascularisation5.
The prespecified 2-year follow-up analysis was therefore undertaken to determine whether these differences persisted over longer-term follow-up and to further clarify the role of QFR in contemporary coronary revascularisation.
How was it executed? The methodology
This prospective, multicentre, randomised trial enrolled patients with at least one angiographically intermediate coronary stenosis (40–90% diameter stenosis by visual estimation) requiring physiological assessment. A total of 2,000 patients from 34 European centres were randomly assigned in a 1:1 ratio to either a QFR-guided or an FFR-guided revascularisation strategy.
Lesions with QFR or FFR values ≤ 0.80 underwent revascularisation, whereas lesions with values > 0.80 were deferred and managed with optimal medical therapy. Both percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) were permitted according to clinical judgement. Clinical outcomes were analysed according to the intention-to-treat principle, and 2-year follow-up was completed in 97.8% of the study population.
The primary endpoint of the original trial was major adverse cardiovascular events (MACE), defined as the composite of all-cause death, myocardial infarction, or unplanned revascularisation at 1 year. The trial was designed to assess whether QFR-guided revascularisation was non-inferior to FFR-guided management.
The present report presents the pre-specified 2-year follow-up analysis, evaluating rates of MACE (defined as the composite of all-cause death, myocardial infarction [MI], and unplanned revascularisation), the individual components of MACE, and the composite endpoint of target vessel failure (TVF; defined as the composite of cardiac death, target vessel MI, and ischaemia-driven target vessel revascularisation).
What is the main result?
Between November 2018 and July 2023, a total of 2,000 patients with angiographically intermediate coronary stenoses were enrolled across 34 European centres and randomised to either QFR-guided or FFR-guided revascularisation. Follow-up at 2 years was completed in 97.8% of patients. QFR classified significantly more lesions as functionally significant than FFR (46.2% vs 38.2%), resulting in a higher number of stent implantations in the QFR group.
- At 2 years, the primary composite endpoint of MACE occurred in 9.7% of patients in the QFR group and 7.4% of patients in the FFR group (HR 1.34, 95% CI: 0.98-1.81; p = 0.064).
- No significant differences were observed between QFR and FFR regarding all-cause mortality (2.6% vs 2.3%; p = 0.60), myocardial infarction (4.3% vs 3.4%; p = 0.26), or unplanned revascularisation (5.1% vs 4.3%; p = 0.37).
- Ischaemia-driven revascularisation of a previously assessed study lesion occurred more frequently in the QFR group than in the FFR group (3.1% vs 1.8%; HR 1.81, 95% CI: 1.00-3.26; p = 0.050).
- Landmark analysis demonstrated that the excess risk associated with QFR was confined to the first year after randomisation. Between years 1 and 2, MACE rates were identical in both groups (3.2% vs 3.2%; HR 0.97, 95% CI: 0.58-1.62; p = 0.92).
- In the per-protocol analysis, QFR guidance remained associated with a significantly higher risk of MACE at 2 years compared with FFR guidance (9.5% vs 6.9%; HR 1.40, 95% CI: 1.02-1.92; p = 0.04).
Critical reading and the relevance for clinical practice:
The FAVOR III Europe trial is the first adequately powered randomised study to directly compare an angiography-based physiological assessment strategy with the current invasive gold standard, FFR. This is particularly important because previous evidence supporting QFR was largely based on diagnostic validation studies and comparisons with angiography-guided PCI rather than head-to-head comparisons with FFR6.
The most relevant finding is that QFR classified more lesions as functionally significant, resulting in substantially higher rates of revascularisation and stent implantation. Despite this more aggressive treatment strategy, clinical outcomes were not improved. In fact, MACE rates remained numerically higher in the QFR group, while the per-protocol analysis demonstrated significantly worse outcomes compared to FFR-guided management. These results are particularly noteworthy when compared with previous physiology trials. In both DEFINE-FLAIR and iFR-SWEDEHEART, iFR achieved clinical outcomes comparable to FFR, supporting the adoption of wire-based resting physiology in routine practice7,8. In contrast, FAVOR III Europe failed to demonstrate similar results for angiography-derived physiology, suggesting that angio-based physiological assessment may still face important limitations compared with pressure-wire-based methods.
These findings should be interpreted alongside the FAVOR III China trial, which demonstrated superiority of QFR-guided PCI over angiography-guided revascularisation and contributed to the inclusion of angiography-derived physiology in contemporary guidelines6. However, FAVOR III Europe addressed a different and arguably more clinically relevant question: whether QFR can safely replace FFR for physiological lesion assessment. Based on the available evidence, routine substitution of FFR with QFR is not currently supported.
Importantly, the excess risk associated with QFR emerged during the first year and persisted at 2 years without evidence of convergence between groups. Although the present analysis was not powered for long-term comparisons, the findings support FFR as the preferred method for physiological lesion assessment. While angiography-based physiology remains an attractive concept, further technological improvements and dedicated outcome trials are required before QFR can be considered a routine alternative to pressure-wire-based assessment.
References
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213-24.
- Fearon WF, Bornschein B, Tonino PA, Gothe RM, Bruyne BD, Pijls NH, Siebert U; Fractional Flow Reserve Versus Angiography for Multivessel Evaluation (FAME) Study Investigators. Economic evaluation of fractional flow reserve-guided percutaneous coronary intervention in patients with multivessel disease. Circulation. 2010;122:2545-50.
- Tu S, Westra J, Yang J, von Birgelen C, Ferrara A, Pellicano M, Nef H, Tebaldi M, Murasato Y, Lansky A, Barbato E, van der Heijden LC, Reiber JHC, Holm NR, Wijns W; FAVOR Pilot Trial Study Group. Diagnostic Accuracy of Fast Computational Approaches to Derive Fractional Flow Reserve From Diagnostic Coronary Angiography: The International Multicenter FAVOR Pilot Study. JACC Cardiovasc Interv. 2016;9:2024-35.
- Hu X, Zhang J, Yang S, Jiang J, Peng X, Lu D, Pan Y, Guo L, Li J, He W, Zhou H, Pu J, Huang J, Jiang F, Liu Q, Song D, Lu L, Cheng Z, Yang B, Ma J, Chen P, Li S, Meng Z, Tang L, Fan Y, Shin ES, Tu S, Nam CW, Fearon WF, Koo BK, Wang J; II study group. Angiography-derived fractional flow reserve versus intravascular ultrasound to guide percutaneous coronary intervention in patients with coronary artery disease (FLAVOUR II): a multicentre, randomised, non-inferiority trial. Lancet. 2025;405:1491-504.
- Andersen BK, Sejr-Hansen M, Maillard L, et al. Quantitative flow ratio versus fractional flow reserve for coronary revascularisation guidance (FAVOR III Europe): a multicentre, randomised, non-inferiority trial. Lancet. 2024;404:1835-46.
- Xu B, Tu S, Song L, Jin Z, Yu B, Fu G, Zhou Y, Wang J, Chen Y, Pu J, Chen L, Qu X, Yang J, Liu X, Guo L, Shen C, Zhang Y, Zhang Q, Pan H, Fu X, Liu J, Zhao Y, Escaned J, Wang Y, Fearon WF, Dou K, Kirtane AJ, Wu Y, Serruys PW, Yang W, Wijns W, Guan C, Leon MB, Qiao S, Stone GW; FAVOR III China study group. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): a multicentre, randomised, sham-controlled trial. Lancet. 2021;398:2149-59.
- Götberg M, Berntorp K, Rylance R, Christiansen EH, Yndigegn T, Gudmundsdottir IJ, Koul S, Sandhall L, Danielewicz M, Jakobsen L, Olsson SE, Olsson H, Omerovic E, Calais F, Lindroos P, Maeng M, Venetsanos D, James SK, Kåregren A, Carlsson J, Jensen J, Karlsson AC, Erlinge D, Fröbert O. 5-Year Outcomes of PCI Guided by Measurement of Instantaneous Wave-Free Ratio Versus Fractional Flow Reserve. J Am Coll Cardiol. 2022;79:965-74.
- Escaned J, Travieso A, Dehbi HM, Nijjer SS, Sen S, Petraco R, Patel M, Serruys PW, Davies J; DEFINE FLAIR Investigators. Coronary Revascularization Guided With Fractional Flow Reserve or Instantaneous Wave-Free Ratio: A 5-Year Follow-Up of the DEFINE FLAIR Randomized Clinical Trial. JAMA Cardiol. 2025;10:25-31.
No comments yet!