07 Apr 2026
Coronary calcification versus thrombus: a deceptive ambiguity revealed in the aftermath of embolisation
#CardioTwitterCase originally published on Twitter
Discriminating between coronary calcification and thrombus in acute settings remains a diagnostic challenge with significant implications for interventional decision-making.
This case was originally published on Twitter by @DrIHHashmi1
Case description
This is a smoker 59-year-old man with diabetes, ischemic heart disease, and a history of previous PCI with stents in the LCx, OM and LAD, who suffered from angina for two or three days. With positive cardiac biomarkers on admission, the patient was admitted on the lines of NSTEACS.
Coronary angiography revealed a short, bifurcating left main (LM) with heavily calcified LAD, and LCx with patent previously placed stents.
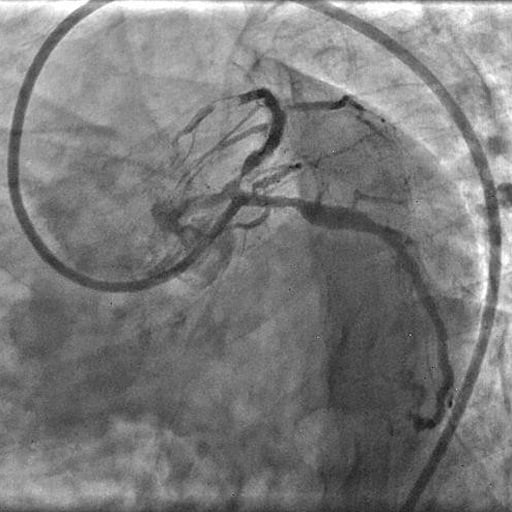
There was significant ostio-proximal disease in both the LAD and LCx, along with total proximal occlusion of the OM branch. Right coronary angiography demonstrated a dominant vessel with extensive calcification and significant stenotic disease involving the proximal, mid, and distal segments.
The patient was initially shifted to the ICU with a plan for multivessel PCI using rotational atherectomy.
However, post-angiography, the patient developed worsening symptoms, accompanied by significant ST-segment elevation in the anterior leads and bradycardia.
The differential diagnosis included acute thrombosis and iatrogenic dissection in the setting of heavy calcification.
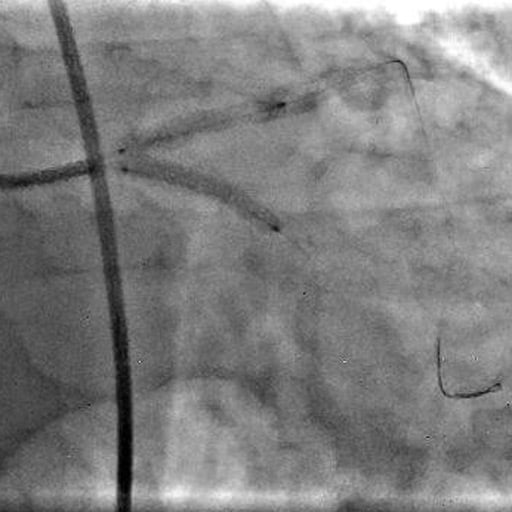
The patient was urgently transferred back to the catheterisation laboratory for revascularisation. A check angiogram prompted reconsideration of the initial strategy (rotational atherectomy vs cutting balloon), as distal thrombus embolisation was noted.
A 3.0 x 6 mm cutting balloon was therefore utilised to modify the calcified lesion. This was followed by simultaneous stenting from the left main to the LAD and LCx (3.0 x 24 mm Promus Elite stents) using the simultaneous kissing stent (SKS) technique.
Post-dilatation was performed using a 4.0 mm non-compliant balloon in both the LAD and LCx, followed by final kissing balloon inflation (4.0 x 10 mm NC balloons at 12 atm), with re-establishment of TIMI 3 flow down the LAD and LCx.
The patient's hospital course was uneventful, and he was discharged after two days with a plan for staged PCI to the RCA at six weeks.
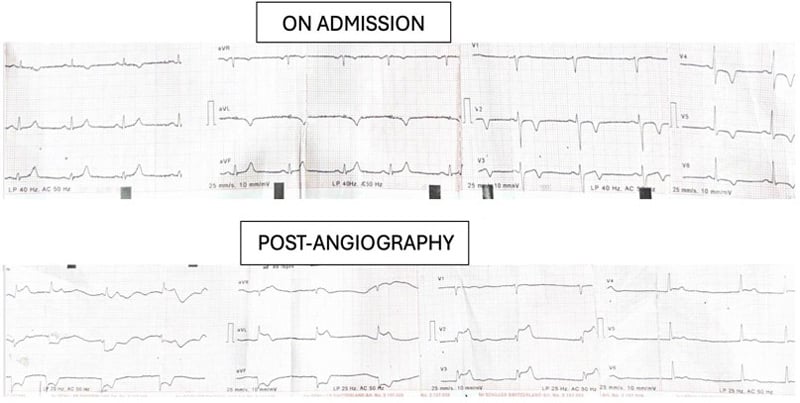
Picture 1: ECG at admission compared with post-angiography, showing significant changes from baseline.

Picture 2: Diagnostic right coronary angiogram showing dominant vessel with extensive calcification and significant stenotic disease involving the proximal, mid, and distal segments

Picture 3: Diagnostic left coronary angiogram showing short, bifurcating left main (LM) with heavily calcified LAD and LCx with patent previously placed stents. There was significant ostio-proximal disease in both the LAD and LCx, along with total proximal occlusion of the OM branch.
Picture 4: Check angiogram demonstrating thrombus embolisation.
Picture 5: Simultaneous stenting from the left main to the LAD and LCx (3.0 × 24 mm Promus Elite stents) using the simultaneous kissing stent (SKS) technique after lesion preparation using a cutting balloon.

Picture 6: Final check injection following post-dilatation showing TIMI III flow across the vessels.
Final remarks
This case exemplifies the deceptive ambiguity of coronary pathology, often challenging initial diagnostic impressions and pre-procedural strategies.
It underscores the critical importance of integrating real-time clinical judgment with multimodality imaging to guide management.
Notably, an unexpected event—embolisation—proved pivotal in unmasking the underlying pathology and ultimately directing successful intervention.
Original tweet and Twitter discussion
What do you think has happened here pic.twitter.com/SRcVJdcXA0
— Dr Imran Hanif Hashmi (@DrIHHashmi1) March 4, 2026
Authors






1 comment
Congratulations on the case. In my opinion, we should proceed with a technical two-stent strategy, possibly using the DK crush technique or mini-crush, placing the first stent in the circumflex artery and performing the crush in the left main, in order to then place the second stent in the LAD. Additionally, in this case I would suggest using intravascular ultrasound or, even better, OCT for optimal stent apposition and expansion. Of course, performing simultaneous deployment of both stents would have been somewhat risky, as the patient could have collapsed. Perhaps the use of Impella CP would have been preferable for this strategy. Nevertheless, the angiographic result is excellent. Congratulations once again!