Side branch additional treatment for coronary bifurcation lesion revascularisation: insights from the KISS randomised trial
Selected in JACC: Cardiovascular Interventions by A. Cader
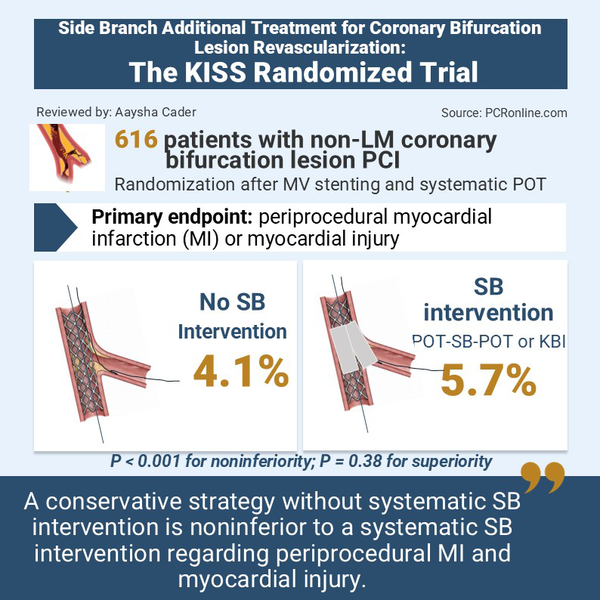
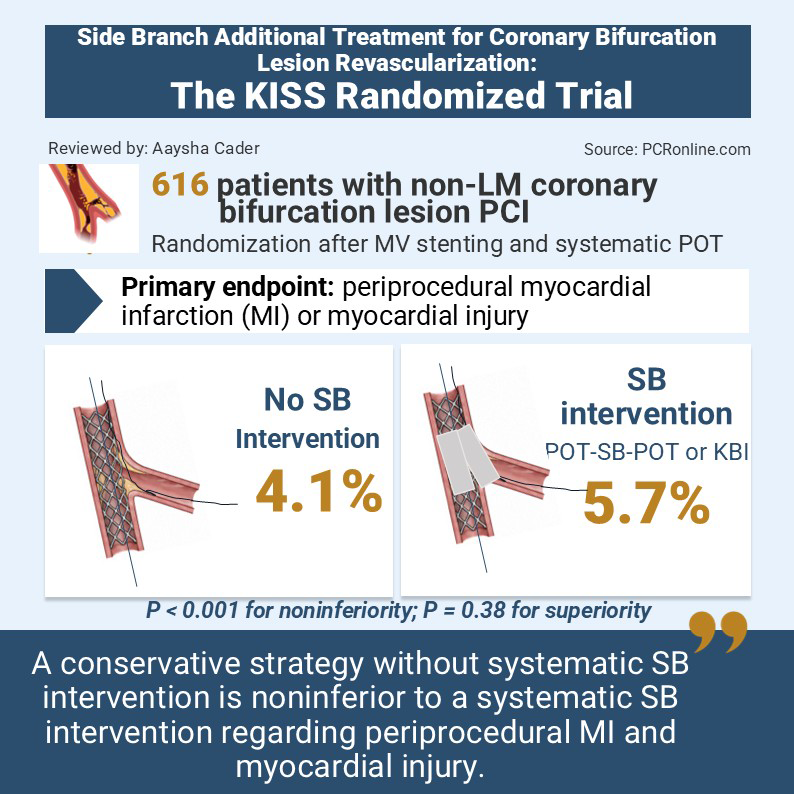
In patients with non-left main coronary bifurcation lesions treated with provisional stenting and POT, the KISS randomised trial compares a strategy of no side branch intervention versus systematic side branch treatment.
References
Authors
Bernard Chevalier, Luc Cornillet, Frederic Bouisset, Laurent Delorme, Stephane Champagne, Philippe Brunel, Katrien Blanchart, Giuseppe Ferrante, Manuel Pan, Pedro Goncalves, Antoinette Neylon, and Benoit Lattuca for the KISS Trial Group
Reference
JACC: Cardiovascular Interventions Volume 19, Number 8 - 19(8):961-972.
Published
27 April 2026
Link
Read the abstractReviewer

My Comment
Why this study – the rationale/objective?
Percutaneous coronary intervention (PCI) for coronary bifurcation lesions (CBL) involves technical challenges, particularly risk for side branch (SB) impairment due to bifurcation carina shift or dissection. Provisional stenting of the main vessel (MV) sized to its distal reference diameter, followed by proximal optimisation technique (POT) is current standard of care1. After these steps, additional side branch intervention (SBI) remains a matter of debate, with previous studies not accounting for the contemporary bifurcation PCI strategy of provisional stenting.
The KISS trial aimed to determine whether, after MV provisional stenting and POT, a conservative strategy of non-intervention of SB was non-inferior to systematic side branch intervention (SBI) in non-left main CBLs2.
How was it executed? The methodology
The KISS trial was a randomised (1:1), prospective, open-label, multicentre, international study. All patients with coronary artery disease (CAD) undergoing revascularisation were considered eligible with the following inclusion criteria:
Inclusion criteria
- Non-left main coronary bifurcation with de novo significant MV lesion (≥ 70% angiographic stenosis and/or FFR ≤ 0.8) requiring MV stenting
- SB diameter ≥ 2.25 mm and compatibility with potential stent implantation
- Absence of SB occlusion or SB slow flow associated with ongoing ischemia after MV POT
Important exclusion criteria:
- LM coronary lesion or CBL requiring a planned double-stenting strategy
- Medina type 0,0,1 bifurcation without planned MV stenting
- Unsuccessful non–target vessel intervention prior to treatment of the target lesion
- SB TIMI flow grade < III
- SB predilatation before randomisation
- Chronic total occlusion of any target vessel
- ST-segment elevation MI or cardiogenic shock
- Left ventricular ejection fraction < 20%.
Systematic wiring of the MB and SB was done at the outset. After appropriate MV lesion preparation, a drug-eluting stent was implanted, sized 1:1 to distal MVB reference diameter, followed by a systematic POT.
Timing of randomisation: after the POT, if there was no SB occlusion or SB slow flow, patients were randomised to no SBI vs SBI. A guidewire must remain in the non-stented vessel until randomisation.
In the SBI group, the intervention was left to the operator’s discretion, and could be one of the following: SB balloon inflation, kissing balloon inflation (KBI), or the POT–SB dilatation–POT technique3.
In case of KBI, a final POT was recommended. In case of POT–SB dilatation–POT technique, a final POT was mandatory.
The primary endpoint was the rate of peri-procedural MI or significant peri-procedural injury according to the Academic Research Consortium-2 (ARC-2) definition4.
All procedures were independently reviewed by a core laboratory.
What is the main result?
A total of 616 patients were randomised: 303 patients in the no-SBI group and 313 patients in the SBI group. Group crossover was observed in 9 patients. The mean age was 67.7 ± 10.9 years, with ¬75% male predominance; 81% had chronic coronary disease.
Baseline clinical characteristics were well-balanced, except for history of previous MI and previous PCI, more frequent in the SBI group.
Procedural characteristics:
Radial access was preferred in ¬90% of procedures in both groups. The left anterior descending coronary artery (LAD)/ diagonal bifurcation was involved in the majority (81.2% of patients).
No significant between-group differences were seen for angiographic characteristics of the treated bifurcation including MV lesion length (¬22mm), MV and SB diameters (¬2.5mm), Medina classification (mostly [1,1,1], [1,1,0] and [0,1,0]), or lesion preparation (mainly non-compliant balloons).
A POT was performed in 94.4% in the no-SBI group and 95.2% in the SB group (P = 0.635). In the no-SBI group, an SB intervention was done in 2.0% of patients (n = 6), including KBI (n = 4), SB ballooning (n = 1), and SB stenting (n = 1) because of SB flow compromise. In the SBI group, SB intervention included isolated balloon inflation in 57 (n = 175) and KBI in 43% of patients (n = 132). SB stenting was needed in 5.8% (n = 18).
Similar technical success was seen in the 2 groups; ¬80% for MV; 100% and 99% for no-SBI and SBI groups, respectively.
SB dissection was more frequent in the SBI group (2.9% vs 0.0%;P = 0.004).
The no-SBI group was associated with shorter procedure time (median 34 minutes vs 45 minutes; P < 0.001), fluoroscopy time (median 10 minutes vs 13 minutes; P < 0.001), reduced radiation dose (453 mGy vs 629 mGy; P < 0.001) and reduced contrast volume(130 mL vs 150 mL; P < 0.001) in the no-SBI vs SBI group respectively.
Endpoints:
Peri-procedural MI or significant myocardial injury occurred in 4.1% (n = 11) in the no-SBI group vs 5.7% (n = 16) in the SBI group (P < 0.001 for noninferiority; P = 0.38 for superiority) in the intention-to-treat cohort; and in 4.1% (n = 11) and 5.9% (n = 16) respectively in the per protocol analysis (P < 0.001 for noninferiority; P = 0.34 for superiority). There were no significant interaction of the primary endpoint with age, sex, Medina classification, or residual SB stenosis degree.
At 1 year, there was no difference in target lesion failure (4.9% vs 6.4% in the no-SBI and SBI groups, respectively; P = 0.442), although the study was not powered for this endpoint. At 1 year, there was improvement in angina status in 99.0% vs 93.7% of patients in the no-SBI and SBI groups, respectively (P = 0.039).
A complementary analysis of only the SBI group found that the use of only SB ballooning was associated with a lower rate of the primary endpoint in comparison with a KBI technique (3.4% vs 8.9% respectively; P < 0.001 for noninferiority), but without a significant difference in clinical secondary endpoints.
Critical reading and the relevance for clinical practice:
This study affirms that no SBI is non-inferior to SBI with respect to periprocedural MI and myocardial injury, in a cohort of patients with non-complex non-left main bifurcation lesions undergoing contemporary bifurcation PCI, including POT.
The randomised NORDIC III (Nordic-Baltic Bifurcation Study III) trial published in 2011 showed that routine KBI had less angiographic restenosis in bifurcation lesions but a lack of overall clinical benefits5. Admittedly, this was conducted prior to routine use of POT, underscoring the relevance of the KISS trial in a contemporary cohort randomised after POT.
Thus, in uncomplicated bifurcation PCI without SB compromise, POT is currently the only recommended intervention after MV stenting1,6 and intervention on the SB appears optional only in case of SB flow impairment or acute occlusion of the SB.
The use of intracoronary imaging was noted to be very low in this trial and it is difficult to say if greater use of imaging might have changed outcomes. Furthermore, the study did not address the use of DCBs to treat SB’s after MV PCI, and this would be interesting, given its efficacy beyond the immediate periprocedural period. Indeed, in the DCB BIF trial, in case of compromised SB after MV stenting, a DCB for the compromised side branch resulted in a lower 1-year rate of the composite outcomes compared to non-compliant balloons, albeit high rates of early periprocedural MI not leading to revascularisation7.
Limitations of the study include open-label design, a lack of standardisation of definitions for periprocedural MI and lower-than-anticipated number of events potentially leading to underpowering of the trial. It is also important to understand which population this trial does not apply to: left main bifurcation, non-left main bifurcations with larger side branches greater than 2.5mm, long and significant SB disease, and complex bifurcation PCI with 2-stent strategies.
References
- Albiero R., Burzotta F., Lassen J.F., et al. Treatment of coronary bifurcation lesions, part I: implanting the first stent in the provisional pathway. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention. 2022;18:5: e362-e376.
- Chevalier B, Cornillet L, Bouisset F, et al; KISS Trial Group. Side Branch Additional Treatment for Coronary Bifurcation Lesion Revascularization: Insights From the KISS Randomized Trial. JACC Cardiovasc Interv. 2026;19(8):961-972.
- Finet G., Derimay F., Motreff P., et al. Comparative analysis of sequential proximal optimizing technique versus kissing balloon inflation technique in provisional bifurcation stenting: fractal coronary bifurcation bench test. JACC Cardiovasc Interv. 2015;8:10: 1308-1317.
- Garcia-Garcia H.M., McFadden E.P., Farb A., et al. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 consensus document. Eur Heart J. 2018;39:23: 2192-2207
- Niemelä M., Kervinen K., Erglis A., et al. Randomized comparison of final kissing balloon dilatation versus no final kissing balloon dilatation in patients with coronary bifurcation lesions treated with main vessel stenting: the Nordic-Baltic Bifurcation Study III. Circulation. 2011;123:1: 79-86.
- Chevalier B., Mamas M.A., Hovasse T., et al. Clinical outcomes of the proximal optimisation technique (POT) in bifurcation stenting. EuroIntervention. 2021;17:11: e910-e918.
- Gao X., Tian N., Kan J., et al. Drug-coated balloon angioplasty of the side branch during provisional stenting: the multicenter randomized DCB-BIF trial. J Am Coll Cardiol. 2025;85:1: 1-15.

No comments yet!