19 Aug 2019
Case study: Entrapment of rota burr
Complications Rotablator
This is the case of a 63 y/o male, who experienced CAD with stenting for LCx 3 years ago, who suffers from hypertension and Diabetes mellitus type 2 and is in the end stage of renal disease with hemodialysis.
Authors
Clinical presentation
History
- 63 y/o male
- CAD with stenting for LCx 3 years ago
- Hypertension
- Diabetes mellitus type 2
- End stage of renal disease with hemodialysis
Presentation
- Chest pain brought on by exertion
- EKG: Sinus rhythm, no obvious ST segment change
- Treadmill test : Diffuse ST segment depression
Diagnostic angiography
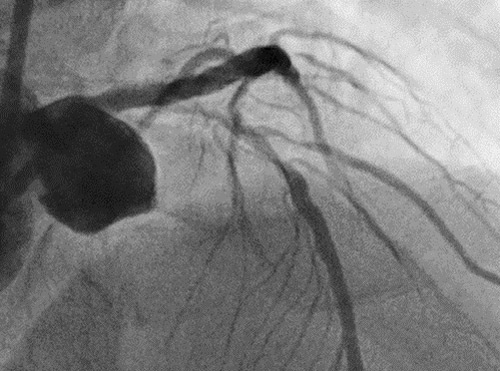
RCA shows diffuse atherosclerosis stenosis lesion, especially at the ostium.
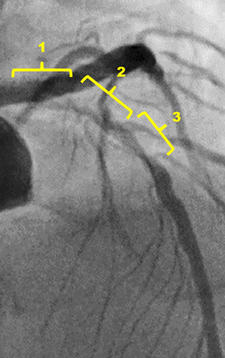
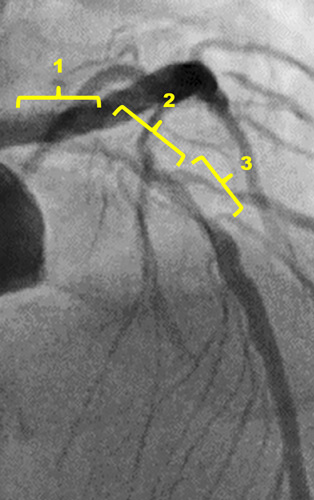
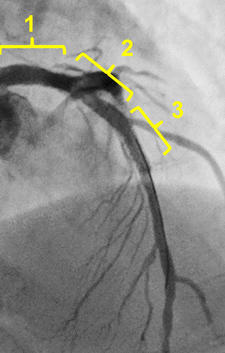
The left coronary artery indicated 90% stenosis with severe calcification from the proximal to the middle part of LAD and diagonal branch
The diagnosis is triple vessel disease and the syntax score is 18. The patient refused bypass surgery.
Target lesion: LAD middle part, Medina (1,1,1)
Strategy: IVUS
- Non compliant balloon
- May use atherectomy
- One provisional stent
The image of IVUS showed 360 degree calcification at the middle part of LAD.
We decided to use rotablation for calcified plaque modification (extra-support wire, 1.5mm burr)
Speed of 180 000 rpm
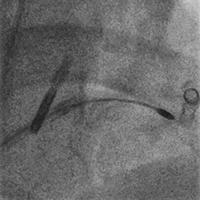
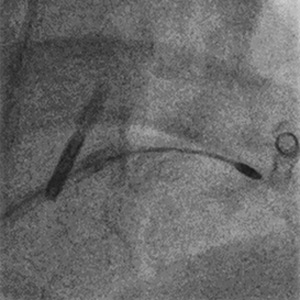
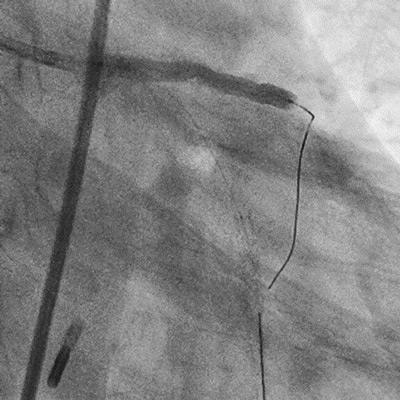
As soon as the lesion was crossed, the rota burr got stuck in the lesion
"Everyone was quiet. All I could hear was my heart beat. The vital sign of the patient was stable then, but I knew I did not have much time..."
Solution No.1
Solution No.2
The patient complained of a tight chest, and a drop in blood pressure was noted.
IABP was inserted, CVS doctors were on standby.
Solution No.3
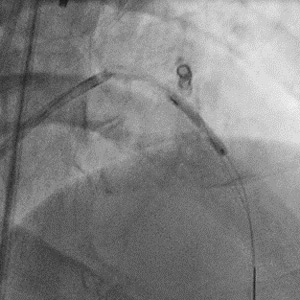
Guideliner 5Fr to remove the rota burr (cut off the drive shaft and sheath) but the tip was too flexible
Solution No.4
ST-01 mother-and-child catheter inserted and the rota burr removed successfully
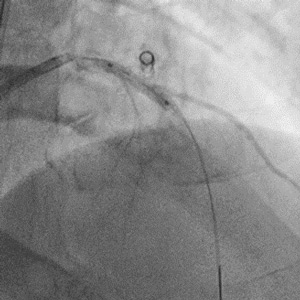
Blood pressure was correct. Non compliant balloon inflation, no extravasation.
One stent strategy
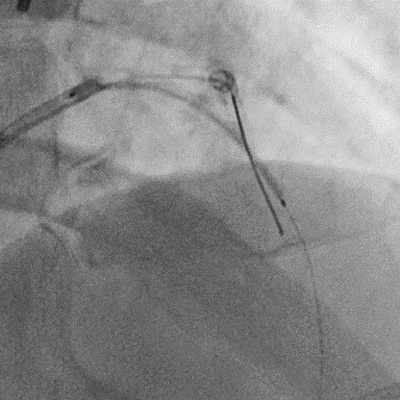
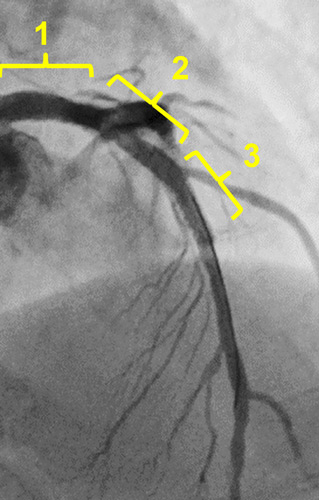
Final angiography
The final IVUS showed stent was apposed correctly and fully expanded.
Follow up
The patient discharged three days later and following an echocardiogram showed adequate LV function.
Conclusion and take-home message
Entrapment of a Rota burr is a rare but serious complication; surgery is often needed. Several bailout techniques are presented in this case. Calcification is always our enemy...
2 comments
Has choice of rota rpm, type of wire and lesion angularity got any role to play in this complication? Or simply the slightly extra forward force noted with folding back of the distal end of the system solely responsible?
I think complications are most important to be anticiapted and prevented. I would add one more important take-home message: in severly calcified lessions in patinets with terminal renal failure, especcialy if you found 360 degree calcium ring on IVUS, always start with the smallest burr (1.25).