01 Jul 2026
From PROTECT-AF to CHAMPION-AF: Where do we stand today?
The evidence for LAA Closure in stroke prevention
In this article, Jens Erik Nielsen-Kudsk reviews the evolution of left atrial appendage closure, from early trials such as PROTECT‑AF to recent evidence including CHAMPION‑AF, and discusses its expanding role in stroke prevention for atrial fibrillation.

Rationale for LAAC
Thrombus formation within the left atrial appendage (LAA) with embolization of thrombotic material to the cerebral or systemic circulation represents the prevailing pathophysiological understanding of stroke and systemic embolism in atrial fibrillation (AF). From this perspective, thromboembolism associated with AF can be viewed as a structural disease process, making LAA closure a logical site-specific strategy for stroke prevention. Thrombus formation within the left atrial cavity itself is uncommon and typically observed only in the setting of severe mitral stenosis or advanced left ventricular dysfunction. Moreover, the randomized ARCADIA trial (n=1,015) demonstrated no benefit of direct oral anticoagulation (apixaban) compared with aspirin in patients with atrial cardiomyopathy and prior stroke1 arguing against the cardiomyopathy/thrombogenic-milieu hypothesis.
The current cornerstone of stroke prevention in AF is treatment with direct oral anticoagulants (DOACs), which reduce the risk of stroke by approximately 60-70%. However, several limitations remain. These include bleeding complications, with rates of major bleeding of approximately 3% per year and clinically relevant non-major bleeding approaching 6-7% per year, as well as undertreatment (>20%), inappropriate dose reduction, non-adherence (>30%), treatment interruptions, renal dysfunction, suboptimal reversal agents and contraindications to thrombolysis in acute ischemic stroke. Notably, approximately half of patients with AF who are admitted with stroke are already receiving DOAC therapy.
Given the rapidly growing population of patients with AF, there is a clear need for more effective stroke prevention strategies. The ultimate goal is to minimize the risk of stroke while avoiding the bleeding burden associated with long-term anticoagulation. LAA closure offers a targeted, non-pharmacological approach to stroke prevention by eliminating the primary source of thrombus formation in AF. In addition, it has the potential to overcome several important limitations of DOAC therapy, including bleeding risk, treatment interruptions, and non-adherence. Percutaneous left atrial appendage closure (LAAC) has primarily been reserved for patients with AF who are unsuitable for long-term oral anticoagulation, but the spectrum for LAAC is being expanded to broader AF populations based on evidence from recent large RCTs.
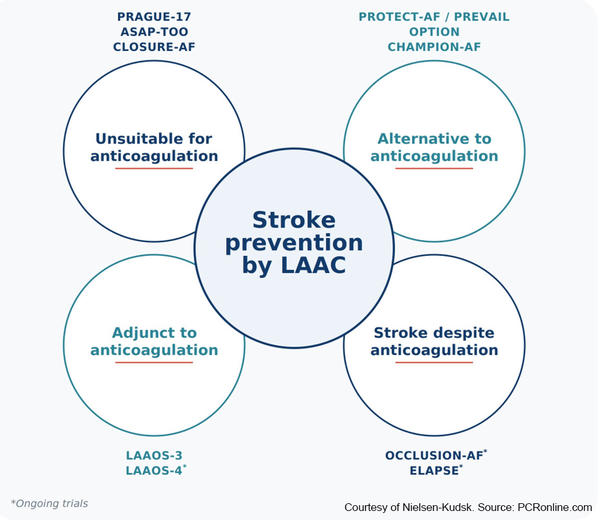
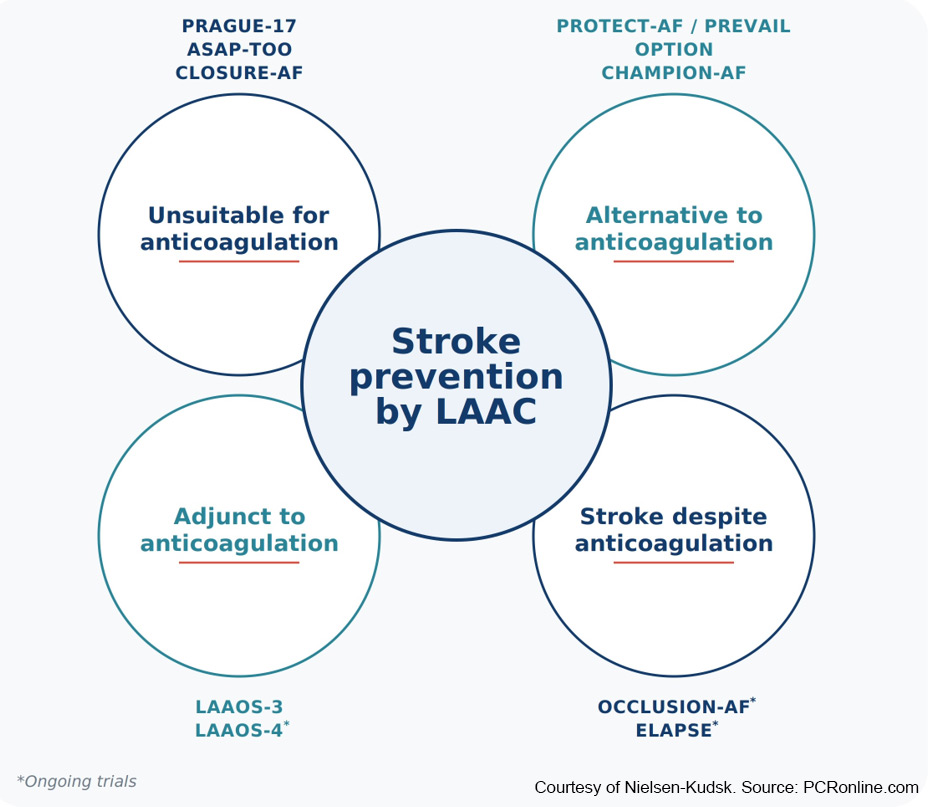
Evidence for stroke prevention by left atrial appendage closure (LAAC)
Courtesy of Jens Erik Nielsen-Kudsk. Source: PCRonline.com
Proof-of-concept for LAAC and procedural safety
PROTECT-AF (n=707) was the first randomized controlled trial and established the proof-of-concept for LAAC.2 Percutaneous LAAC with the Watchman device was shown to be non-inferior to warfarin for the composite endpoint of stroke, systemic embolism, and cardiovascular death. However, the rate of early procedure-related complications was high (8.7%), which led to the subsequent PREVAIL trial, demonstrating a reduction in complication rate to 4.2%.3
Over time, procedural safety has improved substantially, with contemporary rates of approximately 0.5–1% using the Watchman FLX device. Pericardial effusion requiring intervention is now <0.5%, while periprocedural stroke and device embolization are very rare. In current practice, LAAC is considered a low-risk procedure with a safety profile comparable to other established cardiac interventions such as catheter ablation and PCI.
LAAC in AF patients unsuitable for anticoagulation
Although PROTECT-AF and PREVAIL enrolled patients who were generally eligible for anticoagulation, these trials established LAAC as a mechanical stroke prevention strategy, which subsequently led to its predominant use in patients with contraindications to oral anticoagulation or those considered unsuitable for long-term therapy.
The PRAGUE-17 trial (n=402), which enrolled high bleeding-risk patients with atrial fibrillation, demonstrated that LAAC was non-inferior to DOAC for a composite endpoint of stroke, systemic embolism, cardiovascular death, or major bleeding. Importantly, LAAC was associated with a significantly lower rate of long-term bleeding.4
In ASAP-TOO (n=888 planned, n=484 enrolled), LAAC was investigated against SAPT or no treatment in AF patients with a contraindication for OAC. Unfortunately, the trial was stopped before time due to slow enrolment. Follow-up after 5 years showed a stroke/SE event rate of 11.4% in the control group and 7.8% in the LAAC arm (not significant due to lack of power).5
In contrast, the German CLOSURE-AF trial (n=888), which aimed to evaluate LAAC in a similar high-risk population, did not demonstrate non-inferiority of LAAC compared with standard-of-care therapy (approximately 85% DOAC use) for the composite endpoint of stroke, systemic embolism, cardiovascular death, and major bleeding).6 Ischemic stroke rates were similar between groups, but major bleeding was paradoxically higher in the LAAC arm. The enrolled population was highly comorbid, with an annual mortality rate of approximately 14%. A total of 73.6% had renal impairment, and 31.9% had severe renal dysfunction (eGFR <30 ml/min).
A total of 10,872 patients were screened to enrol 888 participants, suggesting substantial selection bias toward a particularly frail and less typical LAAC candidate population. Importantly, LAAC was also reimbursed and performed in clinical practice at participating centers during the trial, which may have influenced enrollment patterns. The observed procedural complication rate was high (5.7%), and the mandated use of dual antiplatelet therapy for three months in the device arm likely contributed to an increased rate of periprocedural bleeding events. Overall, CLOSURE-AF likely reflects outcomes in very elderly, multimorbid, and severely ill patients rather than those typically considered optimal candidates for LAAC in routine clinical practice.
LAAC as an alternative to anticoagulation
In the OPTION trial (n=1,600), left atrial appendage closure (LAAC) using the Watchman FLX device was non-inferior to oral anticoagulation in patients with atrial fibrillation undergoing catheter ablation in a combined endpoint of stroke, SE and death.7 LAAC was performed either concomitantly or within three months following ablation. The incidence of ischemic stroke was very low and similar between groups (approximately 0.4% per year over three years). In contrast, non-procedural major and clinically relevant non-major bleeding was significantly reduced with LAAC compared with oral anticoagulation (8.5% vs 18.1% over three years), corresponding to a 56% relative risk reduction.
The CHAMPION-AF trial (n=3,000) extended these findings to a broader population of patients with atrial fibrillation, demonstrating that LAAC with Watchman FLX was non-inferior to direct oral anticoagulants (DOACs) for the composite endpoint of stroke, systemic embolism, or cardiovascular death (5.7% vs 4.8% over three years).8 Non-procedural major and clinically relevant non-major bleeding was significantly lower with LAAC (10.9% vs 19.0%), representing a 45% relative risk reduction.
When examining individual components of the efficacy endpoint, the rate of ischemic stroke/systemic embolism was slightly higher with LAAC (approximately 1.1% per year) compared with DOAC therapy (0.8% per year). Rates of disabling stroke were low and closely aligned between groups (0.45% vs 0.33% per year, respectively). It is noteworthy that adherence to DOAC therapy in CHAMPION-AF exceeded 85%, which is substantially higher than typically observed in routine clinical practice. In addition, ischemic stroke rates in the pivotal DOAC trials ranged from 1.1% to 1.7% annually, similar to or higher than those observed in CHAMPION-AF.
LAAC as an adjunct to anticoagulation
The LAAOS-3 trial (n=4,770) demonstrated that surgical left atrial appendage occlusion in patients with atrial fibrillation undergoing cardiac surgery reduced the risk of ischemic stroke by 33% in addition to standard anticoagulation.9 This provided strong proof-of-concept for mechanical stroke prevention, and surgical LAA occlusion is now recommended with a Class I indication in AF patients undergoing cardiac surgery.
The ongoing LAAO-4 trial (≈4,000 patients) is evaluating the strategy of combining percutaneous LAAC with DOAC therapy versus DOAC alone in high stroke-risk patients with CHA₂DS₂-VASc scores ≥4. Unlike LAAOS-3, this study employs a fully percutaneous approach to LAA closure.
LAAC in patients with stroke despite anticoagulation
Ischemic stroke despite therapeutic anticoagulation (“breakthrough stroke”) represents an increasing clinical challenge, as these patients carry a particularly high risk of recurrent events (approximately 7–10% per year). Propensity-matched observational studies suggest that LAAC may provide substantial benefit in this setting,10 although more definitive evidence is needed. Ongoing randomized trials, including OCCLUSION-AF and ELAPSE, are expected to further define the role of LAAC in patients experiencing ischemic stroke despite anticoagulation.
Where do we stand today?
Left atrial appendage closure (LAAC) is an established proof-of-concept strategy for stroke prevention in AF, directly aligned with the underlying pathophysiology of thromboembolism in AF. It provides an effective option for stroke prevention in patients who cannot tolerate or adhere to long-term oral anticoagulation.
Recent large randomized trials, including OPTION and CHAMPION-AF, have expanded the evidence base by demonstrating that LAAC may also serve as a viable alternative to direct oral anticoagulants (DOACs), both in patients undergoing AF ablation and in broader “all-comer” AF populations.
LAAC should therefore be considered within a shared decision-making framework, taking into account individual patient factors such as lifestyle, likelihood of long-term medication adherence, bleeding risk, occupational considerations, comorbidities, anticipated need for temporary interruption of therapy, and concomitant medications.
In patients with very high thromboembolic risk, as well as those experiencing ischemic stroke despite therapeutic anticoagulation, ongoing studies will further clarify the role of LAAC, including its potential use as an adjunct to anticoagulation.
References
- Kamel H, Longstreth WT, Tirschwell DL, Kronmal RA, Marshall RS, Broderick JP, et al. Apixaban to Prevent Recurrence After Cryptogenic Stroke in Patients With Atrial Cardiopathy. JAMA. 2024 Feb 20;331(7):573–81. doi:10.1001/jama.2023.27188 PubMed PMID: 38324415; PubMed Central PMCID: PMC10851142.
- Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009 Aug 15;374(9689):534–42. doi:10.1016/S0140-6736(09)61343-X PubMed PMID: 19683639.
- Reddy VY, Doshi SK, Kar S, Gibson DN, Price MJ, Huber K, et al. 5-Year Outcomes After Left Atrial Appendage Closure. JACC. 2017 Dec 19;70(24):2964–75. doi:10.1016/j.jacc.2017.10.021
- Osmancik P, Herman D, Neuzil P, Hala P, Taborsky M, Kala P, et al. 4-Year Outcomes After Left Atrial Appendage Closure Versus Nonwarfarin Oral Anticoagulation for Atrial Fibrillation. Journal of the American College of Cardiology. 2022 Jan 4;79(1):1–14. doi:10.1016/j.jacc.2021.10.023
- Reddy VY, Buchbinder M, Nair DG, Issa ZF, Betts TR, Schmidt B, et al. Long-term outcomes after left atrial appendage closure in anticoagulation-ineligible atrial fibrillation patients: The randomized clinical trial ASAP-TOO. Heart Rhythm. 2026 Apr;S1547527126021752. doi:10.1016/j.hrthm.2026.03.1920
- Landmesser U, Skurk C, Kirchhof P, Lewalter T, Hartung J, Rroku A, et al. Left Atrial Appendage Closure or Medical Therapy in Atrial Fibrillation. N Engl J Med. 2026 Mar 18;NEJMoa2513310. doi:10.1056/NEJMoa2513310
- Wazni OM, Saliba WI, Nair DG, Marijon E, Schmidt B, Hounshell T, et al. Left Atrial Appendage Closure after Ablation for Atrial Fibrillation. N Engl J Med. 2025 Apr 3;392(13):1277–87. doi:10.1056/NEJMoa2408308 PubMed PMID: 39555822.
- Doshi SK, Kar S, Nair DG, Waggoner T, Agarwal H, Moussavian M, et al. Left Atrial Appendage Closure or Anticoagulation for Atrial Fibrillation. N Engl J Med. 2026 Jun 4;394(21):2083–94. doi:10.1056/NEJMoa2517213
- Whitlock RP, Belley-Cote EP, Paparella D, Healey JS, Brady K, Sharma M, et al. Left Atrial Appendage Occlusion during Cardiac Surgery to Prevent Stroke. N Engl J Med. 2021 Jun 3;384(22):2081–91. doi:10.1056/NEJMoa2101897
- Maarse M, Seiffge DJ, Werring DJ, Boersma LVA, STR-OAC LAAO Group, et al. Left Atrial Appendage Occlusion vs Standard of Care After Ischemic Stroke Despite Anticoagulation. JAMA Neurol. 2024 Sep 23;81(11):1150–8. doi:10.1001/jamaneurol.2024.2882
