Very small LAA with a challenging closure
Recurrent strokes despite anticoagulation, a failed first attempt at left atrial appendage closure (LAAC), and a challenging small chicken-wing anatomy: this case brings together several factors that complicate procedural planning and device selection.
In a 65-year-old woman with paroxysmal atrial fibrillation, pre-procedural TOE and CT imaging highlighted the anatomical challenges facing the Heart Team after an unsuccessful implantation of a 20 mm single-disc occluder.
What strategy would you choose to achieve successful LAA closure in this demanding case?
Author

Learning objectives
- To learn how to perform LAAC in challenging anatomies
- To learn how to use CT-scan and 3D TOE for planning
- To understand value of different devices in complex anatomies
Patient description
A 65-year-old woman with paroxysmal atrial fibrillation and prior recurrent strokes despite anticoagulation referred to us for left atrial appendage closure after a failed first attempt in another center.
In 2022, she suffered prior brainstem stroke with acute distal syndrome, dizziness, and tendency to fall to the left (on Lixiana)
In 2020, she had a history of transient ischemic attack in the vertebrobasilar circulation
She presented with:
- CHA₂DS₂-VA Score of 3
- Irritable bowel syndrome
- hypothyroidism
- restless legs syndrome
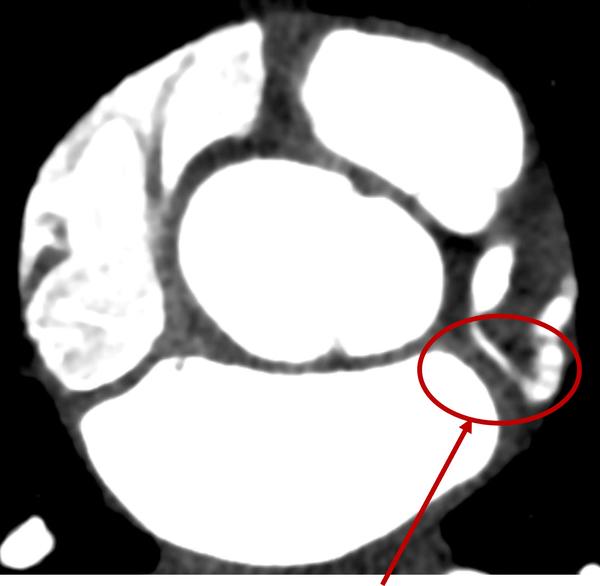
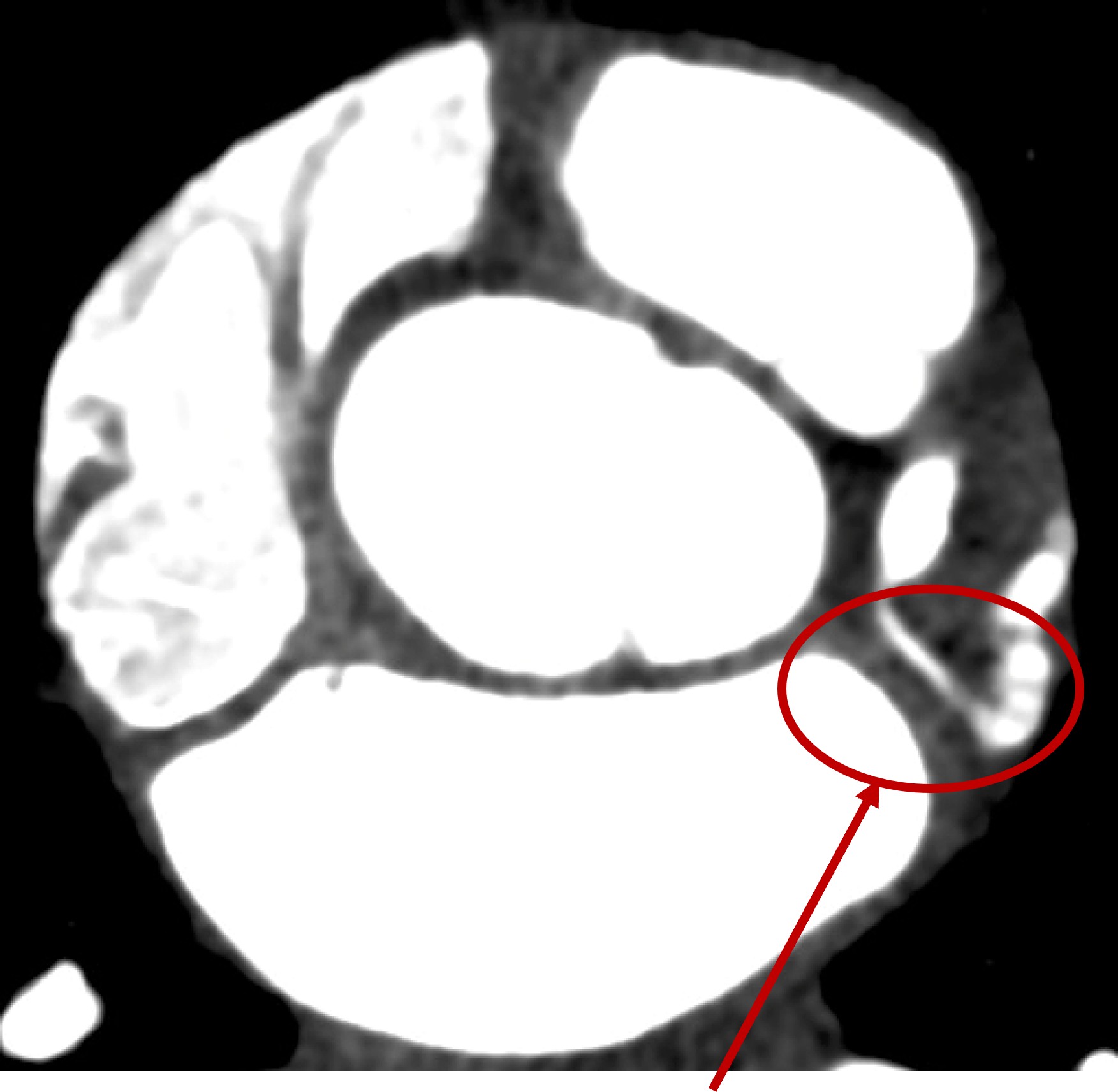
Previous attempt
Protrusion
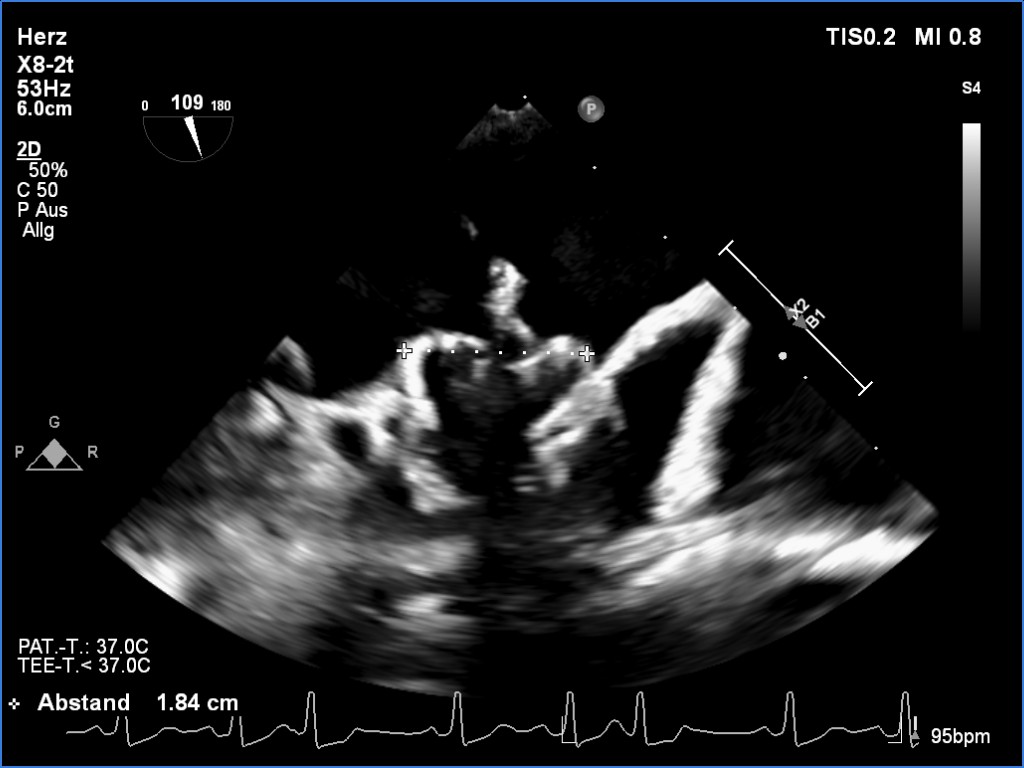
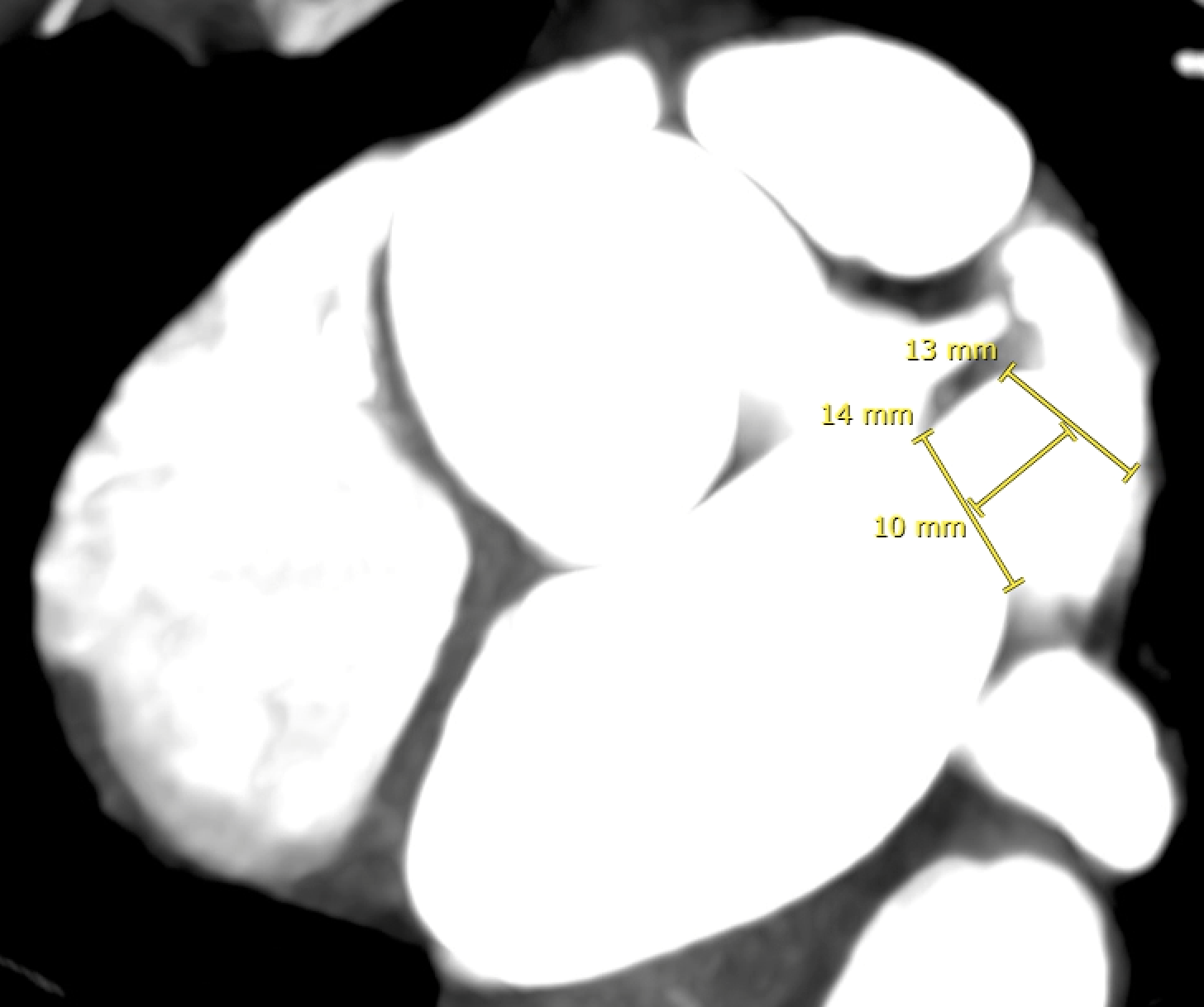
CT measurements in our center
Ostium 17 mm, landing zone 12 mm
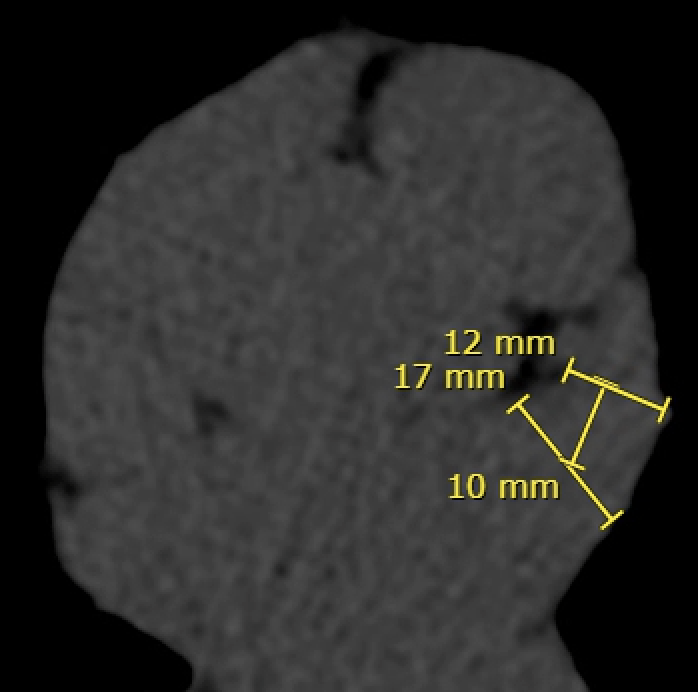
Landing zone (LCX)
CT measurements
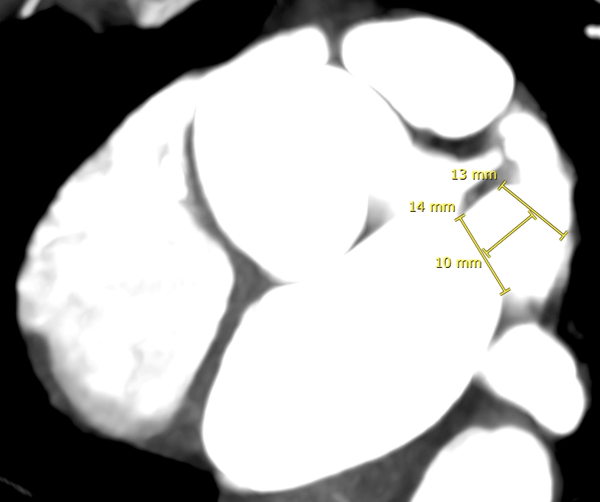
Min/max diameter: 11/13 mm - Average diameter: 12 mm
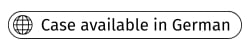
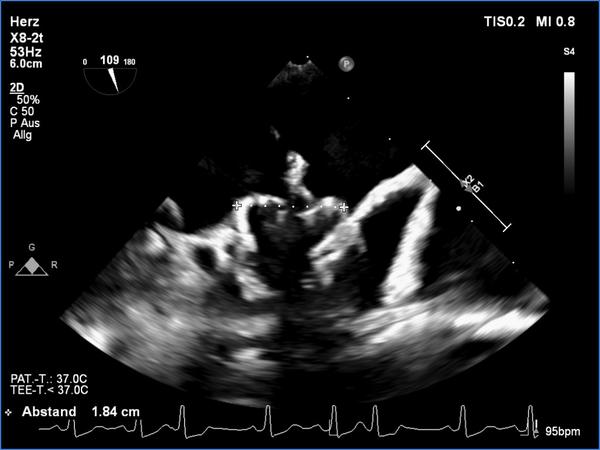
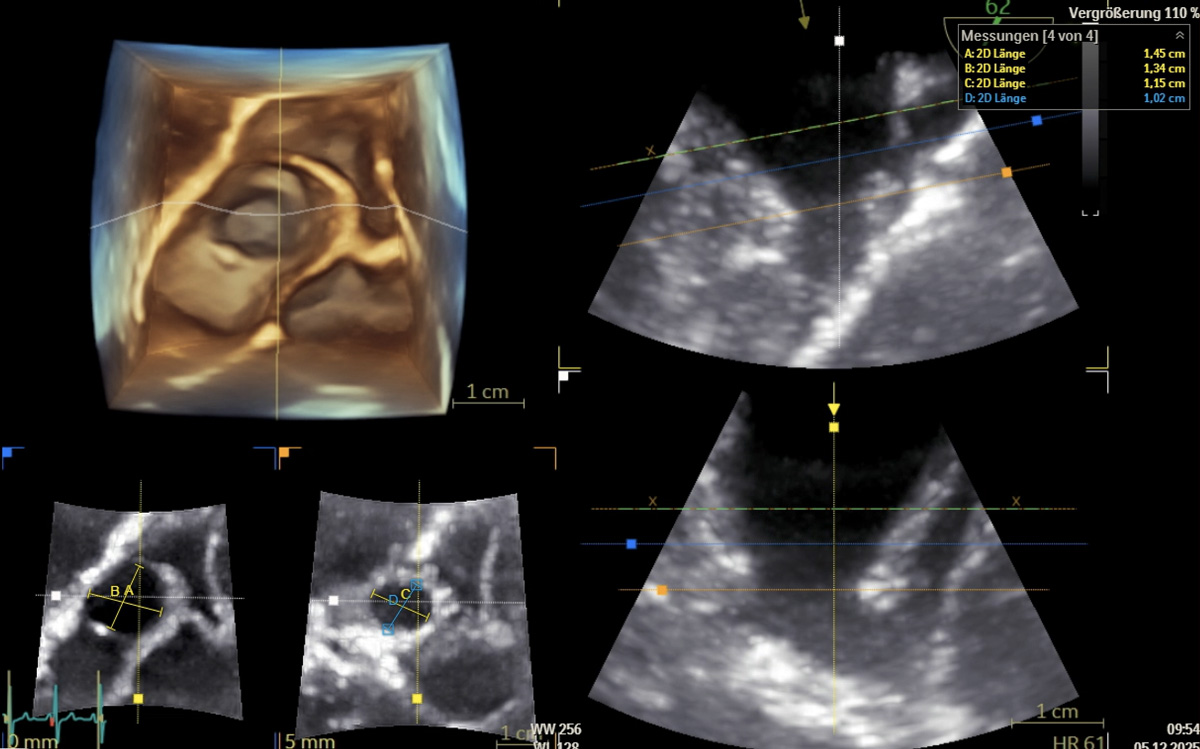
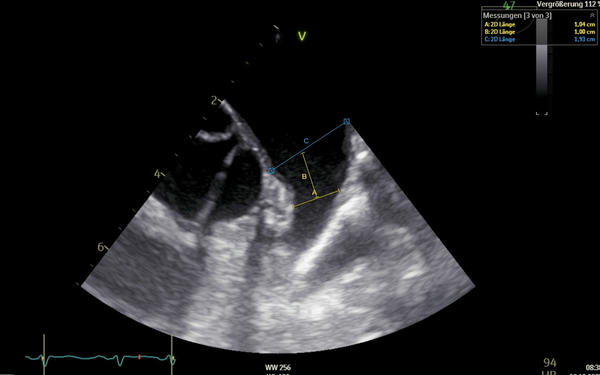
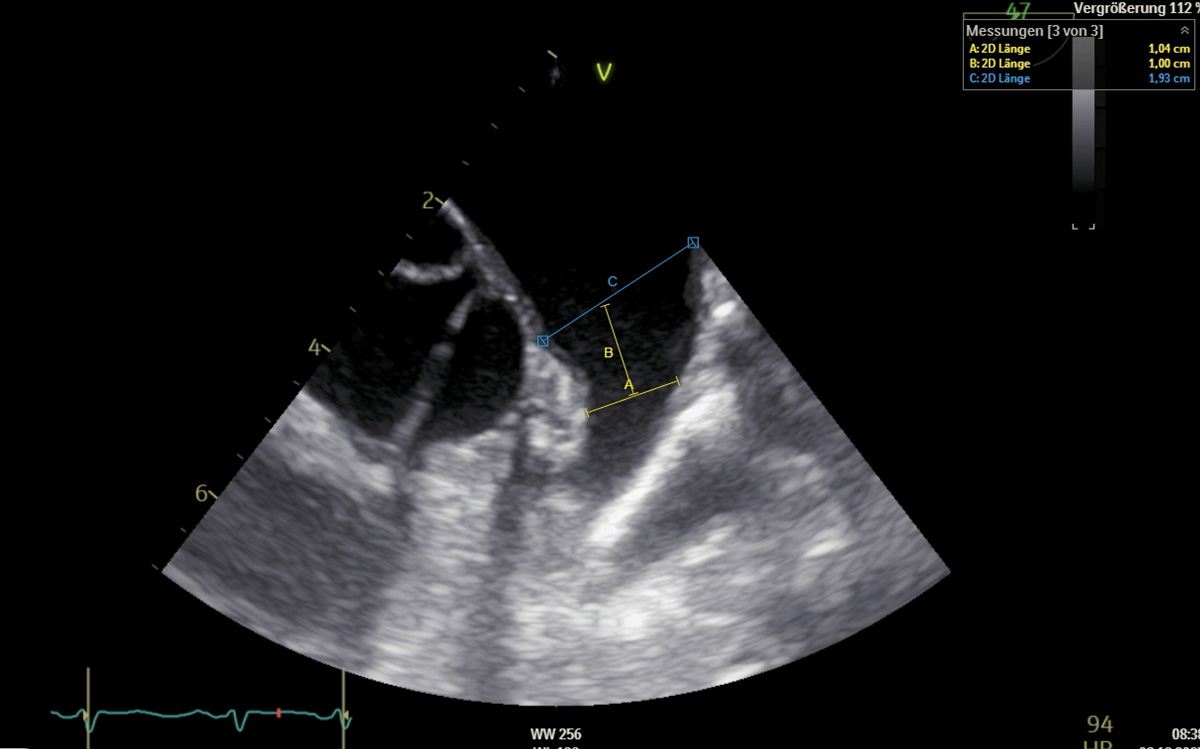
TOE
TOE measurements
- TOE min/max diameter: 10/11 mm and 13/14 mm
- Average diameter: 12 mm

FlexiSlice
Dr. Hamidani declares the following disclosures:
- Receipt of honoraria or consultation fees - Asahi Intecc
- Receipt of honoraria or consultation fees - Shockwave Medical
- Receipt of honoraria or consultation fees - Biotronik
- Receipt of honoraria or consultation fees - Johnson & Johnson MedTech
- Receipt of honoraria or consultation fees - Abbott
No comments yet!