17 Jan 2023
High-speed rotational atherectomy versus modified balloons for plaque preparation of severely calcified coronary lesions: two-year outcomes of the randomised PREPARE-CALC trial
Selected in EuroIntervention Journal by A. Nazmi Calik , I. Polat Canbolat
The PREPARE-CALC trial was the first trial that compared lesion preparation using rotational atherectomy (RA) prior to sirolimus-eluting stent (SES) implantation with modified balloons (MB; cutting or scoring) in patients presenting with chronic coronary syndromes.
References
Authors
Abdelhakim Allali, Gert Richardt, Ralph Toelg, Karim Elbasha, Dmitriy S. Sulimov, Adnan Kastrati, Volker Geist, Mohamed El-Mawardy, Tobias Rheude, Mohamed Abdel-Wahab
Reference
10.4244/EIJ-D-22-00677
Published
27 Decembre 2022
Link
Read the abstract
Reviewers


Our Comment
Why this study – the rationale/objective?
The need for complex coronary percutaneous interventions is growing because of the older population with multiple co-morbidities. Calcified coronary arteries can be found in nearly 10 % of the patients undergoing coronary interventions and are associated with adverse cardiovascular events1. Calcium modifying strategies have been on the ascendant due to new gadgets on the market and changes in patient characteristics. Calcified lesion preparation with balloon-assisted or atherectomy allows successful stent implantation.
The PREPARE-CALC trial was the first trial that compared lesion preparation using rotational atherectomy (RA) prior to sirolimus-eluting stent (SES) implantation with modified balloons (MB; cutting or scoring) in patients presenting with chronic coronary syndromes. At nine months, procedural success was significantly more common with RA, but in-stent lumen loss was comparable between the groups2.
This analysis reviews the 2-year clinical results of the randomized PREPARE-CALC trial.
How was it executed? - the methodology
Two hundred patients with complex calcified coronary lesions and documented ischemia were randomly assigned to either rotational atherectomy (RA) or modified balloons (MB; cutting or scoring) followed by sirolimus-eluting stent (SES) implantation. The principal endpoint of this analysis was target vessel failure (TVF) at 2-year clinical follow-up, defined as the composite of cardiac death, target vessel-related myocardial infarction (MI) or clinically driven target vessel revascularisation (TVR). Major adverse cardiac events (MACE) were a composite of all-cause death, MI or TVR.
What is the main result?
Figure 1. Clinical outcome at 2 years. Kaplan-Meier curves for the cumulative incidence of (A) TVF, (B) MACE and (C) TLR at 2 years in patients undergoing lesion preparation using rotational atherectomy versus modified balloons. MACE: major adverse cardiac events; MB: modified balloon; RA: rotational atherectomy; TLR: target lesion revascularisation; TVF: target vessel failure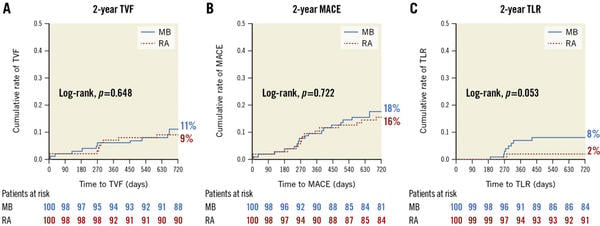
Source: EuroIntervention
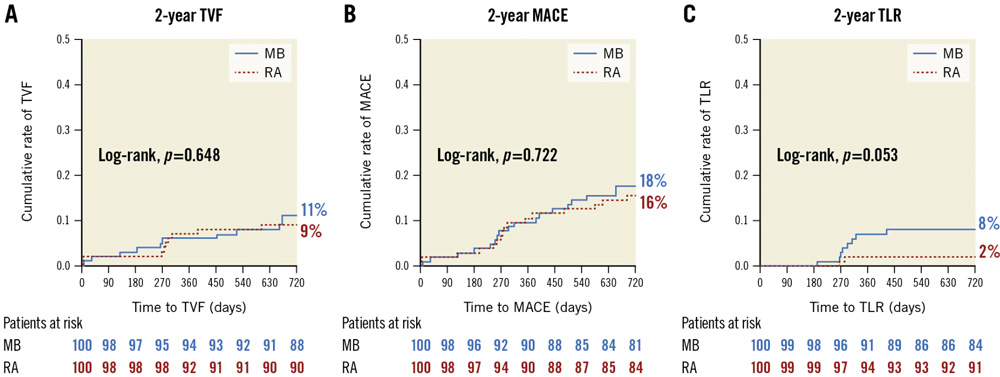
Clinical follow-up at two years was completed in 97 % of the study population. Overall, the cumulative incidence of TVF was 11 % in the MB group vs 9 % in the RA group. (HR 1.23, 95 % [CI]: 0.51–2.96; p = 0.648) (Figure 1A).
The individual components of MACE, all-cause death, TVR and MI, were comparable between both groups and resulted in similar MACE rates (18 % vs 16 %, HR 1.13, 95 % CI: 0.58–2.22; p = 0.722). Of note, a higher rate of TLR was observed in the MB group (p = 0.053) (Figure 1A).
Multivariate analysis showed that only diabetes mellitus was associated with TVF at clinical follow-up (HR 3.67, 95 % CI: 1.04–12.85; p = 0.043). Ostial location and lesion length were independently associated with the time-dependent occurrence of TLR. Additionally, a significant interaction between treatment strategy and lesion length favouring RA in the subgroup of patients with long lesions (≥ 27 mm) and MB in patients with short lesions (< 27 mm) was observed.
Critical reading and the relevance for clinical practice
Calcified coronary lesions are challenging to treat and open to procedural and long-term complications. Heavily calcified lesions have been shown as an independent predictor of mortality irrespective of treatment strategy in a SYNTAXES (Synergy Between PCI With TAXUS and Cardiac Surgery Extended Survival) sub-group study1.
While treating a calcified lesion, caution should be given to proper lesion preparation and optimal stent apposition. The results PREPARE-CALC study offers are comparable and better-than-predicted outcomes with the MB and RA strategies at a 2-year clinical follow-up. The authors explained these excellent results as a consequence of using new-generation DES, intravascular imaging guidance and operator experience in treating calcified coronary lesions.
According to the long-term results of the PREPARE-CALC study, it appears more practical to prefer RA to prepare diffuse calcified lesions, whereas scoring or cutting balloons for shorter ones.
The results of the ongoing ECLIPSE trial3, which aims to evaluate whether a vessel preparation strategy of routine orbital atherectomy system is superior to conventional balloon angioplasty prior to implantation of drug-eluting stents in severely calcified coronary artery lesions, will provide further insight to existing knowledge.
References
- Kawashima H, Serruys PW, Hara H, Ono M, Gao C, Wang R, Garg S, Sharif F, de Winter RJ, Mack MJ, Holmes DR, Morice MC, Kappetein AP, Thuijs DJFM, Milojevic M, Noack T, Mohr FW, Davierwala PM, Onuma Y; SYNTAX Extended Survival Investigators. 10-Year All-Cause Mortality Following Percutaneous or Surgical Revascularization in Patients With Heavy Calcification. JACC Cardiovasc Interv. 2022 Jan 24;15(2):193-204. doi: 10.1016/j.jcin.2021.10.026. Epub 2021 Dec 29. PMID: 34973904.
- Abdel-Wahab M, Toelg R, Byrne RA, Geist V, El-Mawardy M, Allali A, Rheude T, Robinson DR, Abdelghani M, Sulimov DS, Kastrati A, Richardt G. High-Speed Rotational Atherectomy Versus Modified Balloons Prior to Drug-Eluting Stent Implantation in Severely Calcified Coronary Lesions. Circ Cardiovasc Interv. 2018 Oct;11(10):e007415. doi: 10.1161/CIRCINTERVENTIONS.118.007415. Erratum in: Circ Cardiovasc Interv. 2018 Oct;11(10):e000040. PMID: 30354632.
- Généreux P, Kirtane AJ, Kandzari DE, Armstrong EJ, Krucoff MW, Redfors B, Ben-Yehuda O, Lerew DR, Ali ZA, Maehara A, O'Neill WW, Stone GW. Randomized evaluation of vessel preparation with orbital atherectomy prior to drug-eluting stent implantation in severely calcified coronary artery lesions: Design and rationale of the ECLIPSE trial. Am Heart J. 2022 Jul;249:1-11. doi: 10.1016/j.ahj.2022.03.003. Epub 2022 Mar 12. PMID: 35288105.

