03 Apr 2023
Ticagrelor or prasugrel versus clopidogrel in patients undergoing percutaneous coronary intervention for chronic coronary syndromes
Selected in EuroIntervention by A. Nazmi Calik , I. Polat Canbolat
The present study showed that compared to clopidogrel, ticagrelor and prasugrel have comparable 1-year efficacy and safety profiles in individuals with CCS undergoing PCI.
References
Authors
Anoop N. Koshy, Gennaro Giustino, Samantha Sartori, Amit Hooda, Yihan Feng, Clayton Snyder, Shabitri Dasgupta, Kartik R. Kumar, Parasuram Krishnamoorthy-Melarcode, Joseph Sweeny, Sahil Khera, Gregory W. Serrao, Raman Sharma, George Dangas, Annapoorna S. Kini, Roxana Mehran, Samin K. Sharma
Reference
EuroIntervention 2023;18:1244-1253. DOI: 10.4244/EIJ-D-22-00654
Published
20 March 2023
Link
Read the abstract
Reviewers


Our Comment
Why this study – the rationale/objective?
ESC Guidelines for the diagnosis and management of chronic coronary syndromes (CCS)1 recommends prasugrel or ticagrelor usage for high-risk elective percutaneous coronary intervention (PCI) as an expert opinion with a Class IIb-C indication. Real-world data shows that prasugrel and ticagrelor are more frequently prescribed off-label in CCS patients.
In this study, the authors defined the prescription patterns for prasugrel and ticagrelor. They sought to compare the efficacy and safety of clopidogrel versus ticagrelor or prasugrel in a real-world population undergoing elective PCI.
How was it executed? - the methodology
Consecutive patients undergoing PCI for CCS at Mount Sinai Hospital between 2014 and 2019 were enrolled in the study.
The primary efficacy endpoint was the composite of all-cause death and myocardial infarction (MI) (Type-1) at 1 year.
The primary safety outcome was defined as any bleeding occurring during hospitalisation for the index PCI associated with a haemoglobin decrease of >3 g/dL, blood transfusion, or requiring procedural intervention or surgery at the bleeding site, or a bleeding event requiring either hospitalisation or a blood transfusion.
Secondary endpoints included rates of target lesion revascularisation (TLR), stent thrombosis, stroke, and the incidence of the individual components of the primary endpoint.
What is the main result?
A total of 11,508 patients were included in the final analysis. Clopidogrel was the most commonly used P2Y12 inhibitor (8,648 [75.1 %]), followed by ticagrelor (1,717 [14.9 %]) and prasugrel (1,143 [10.0 %]). The mean age was 66 years, and 26.8 % were female. The majority of patients (80.9 %) underwent PCI with femoral access, and 35.7 % of interventions were complex PCI.
Clinical outcomes
The primary efficacy endpoint, composite of death or MI, occurred in 68 (2.7 %) patients in the clopidogrel group, and 223 (3.1 %) patients who received potent P2Y12 inhibitors. (Adj. HR 1.19, 95 % CI: 0.84-2.66, p = 0.32). The rate of bleeding as the primary safety outcome was also similar between the groups (Adj. HR 0.92, 95 % CI: 0.54-1.58, p = 0.76).
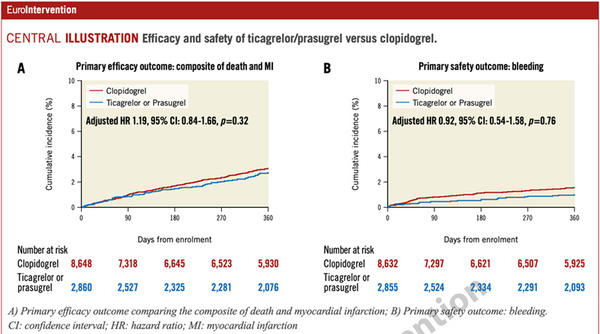
Central illustration: Efficacy and safety of ticagrelor/prasugrel versus clopidogrel - Source: EuroIntervention

As for key secondary endpoints, no difference in stroke or stent thrombosis was noted. Clinically indicated TLR occurred in 159 (6.4 %) and 359 (5.1 %) patients treated with ticagrelor/prasugrel and clopidogrel, respectively (Adj. HR 0.99, 95% CI: 0.74-1.31; p = 0.92).
Factors affecting P2Y12 therapy choice:
Ticagrelor/prasugrel was prescribed significantly higher for patients with complex anatomy (left main PCI: OR 1.80, 95 % CI:1.48-2.19; p < 0.001), complex lesions (bifurcation: OR 1.31, 95 % CI: 1.17-1.46; p < 0.001; lesion length: OR 1.01, 95 % CI: 1.00-1.01; p < 0.001) and complex procedure (number of lesions treated: OR 1.22, 95 % CI: 1.12-1.33; p < 0.001; rotational atherectomy: OR 1.14, 95 % CI: 1.00-1.30; p = 0.04).
Clopidogel-prescribed patients were older and had a higher prevalence of prior cerebrovascular disease, coronary artery bypass grafts, chronic kidney disease and a history of cancer (all p < 0.05).
Critical reading and the relevance for clinical practice
The present study showed that compared to clopidogrel, ticagrelor and prasugrel have comparable 1-year efficacy and safety profiles in individuals with CCS undergoing PCI. The study also showed a trend of preferring prasugrel/ticagrelor over clopidogrel across the study period. This off-label prescribing pattern likely reflects real-world preferences, especially in complex PCI, but there were no differences across subgroups, including among patients that underwent complex PCI.
Further studies are needed to assess whether using the more potent P2Y12 inhibitors in a subset of patients with a high thrombotic and low bleeding risk offers potential advantages over clopidogrel in a CCS population undergoing PCI.
Reference
- Knuuti J, Wijns W, Saraste A. et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020 Jan 14;41(3):407-477.