Coronary vasomotor dysfunction is associated with cardiovascular events in patients with nonobstructive coronary artery disease
Selected in JACC: Cardiovascular Interventions by L. Koliastasis , N. Ryan
In this large single centre registry investigators demonstrated that with the exception of endothelium independent epicardial coronary artery dysfunction, CVDys diagnosed by interventional functional assessment is correlated with adverse cardiac and cerebrovascular events.
References
Authors
Yoshihisa Kanaji, Ali Ahmad, Jaskanwal Deep Singh Sara, Ilke Ozcan, Nadia Akhiyat, Abhiram Prasad, Claire E. Raphael, Tsunekazu Kakuta, Lilach O. Lerman, and Amir Lerman
Reference
J Am Coll Cardiol Intv. 2024 Feb, 17 (4) 474–487
Published
17 February 2024
Link
Read the abstractReviewers


Our Comment
Designed by Leonidas Koliastasis
Why this study – the rationale/objective?
Up to 50 % of all patients referred for angiography due to angina have no obstructive coronary artery disease (ANOCA). In this group, poorer cardiovascular outcomes have been demonstrated.
Coronary vasomotor dysfunction (CVDys) can be classified by anatomical and functional mechanisms; endothelium-dependent microvascular and epicardial coronary dysfunction, and endothelium-independent microvascular and epicardial coronary dysfunction.
This retrospective study sought to evaluate the clinical outcomes in patients with ANOCA classified by CVDys phenotype.
How was it executed – the methodology?
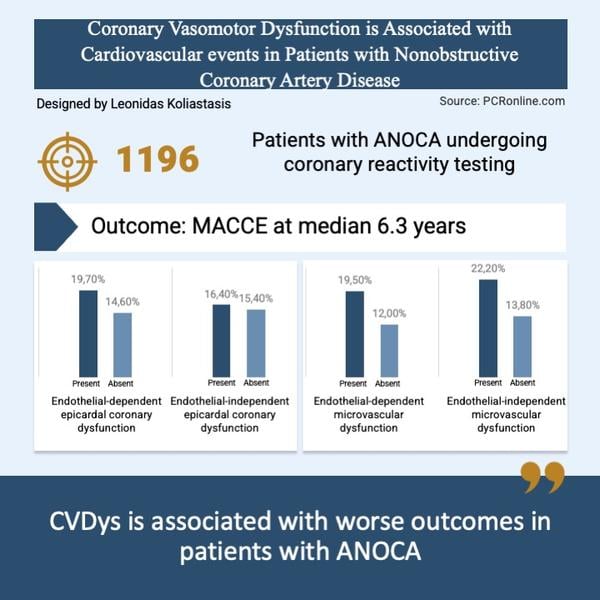
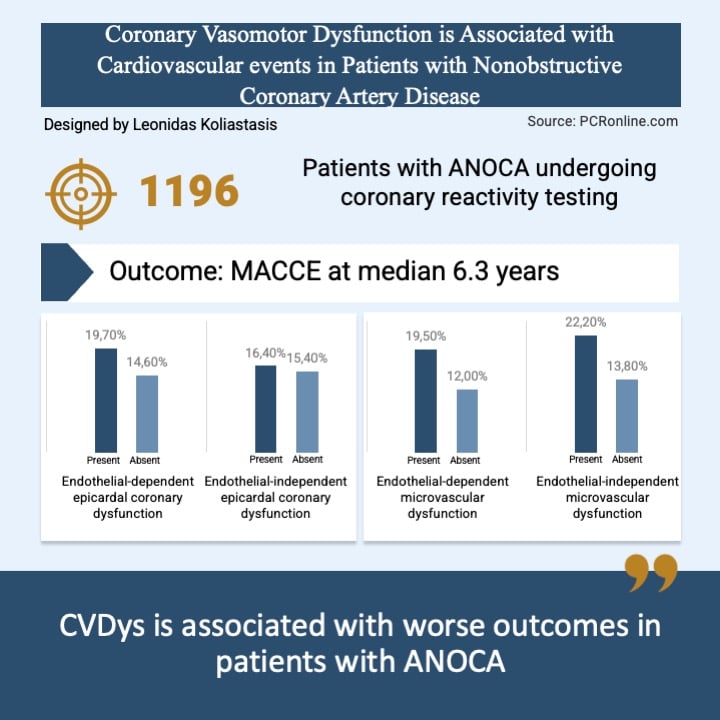
This retrospective study included 1,196 patients with ANOCA who underwent coronary reactivity testing (CRT) from 1997-2021 at a single institution.
Following angiography, a doppler wire and coronary infusion microcatheter were placed in the LAD, intracoronary bolus injections of incremental doses (18-72 μg) of adenosine were administered to induce maximal hyperaemia. Coronary flow reserve (CFR) was calculated by dividing the average peak coronary flow velocity (APV) during maximal hyperaemia by the baseline APV.
Acetylcholine was then infused selectively into the LAD, 10−6, 10−5, and 10−4 mol/L at 1 mL/min for 3 minutes at each concentration. Doppler measurements of peak velocity were performed after each Ach infusion, followed by repeat coronary angiography. Coronary artery diameter in the mid-LAD was measured at baseline and after Ach infusion.
Coronary blood flow (CBF) in the LAD was calculated from the Doppler-derived time-velocity integral and vessel diameter, using the formula: CBF = π × (coronary artery diameter/2)2 × (APV/2). The maximal percentage change in CBF in response to Ach infusion (%ΔCBF-Ach) compared with CBF at baseline was then calculated.
Intracoronary nitroglycerin (NTG) 200 μg was administered and coronary artery diameter and percentage change in cross-sectional area in response to intracoronary NTG administration (%ΔCSA-NTG) were measured.
Four CVDys phenotypes were identified:
- Endothelium-independent microvascular dysfunction: coronary flow reserve (CFR) < 2.5
- Endothelium-dependent microvascular dysfunction: a <50% increase in coronary blood flow after Acetylcholine (Ach) infusion.
- Endothelium-dependent epicardial coronary artery dysfunction coronary artery vasoconstriction with a percentage change in coronary artery diameter in response to Ach infusion (%ΔCAD-Ach) of < 20 %.
- Endothelium-independent epicardial coronary artery dysfunction: a percentage change in cross sectional area in response to intracoronary nitroglycerin (%ΔCSA-NTG) of < 20 %
The outcome of interest was MACCE, CV death, nonfatal MI, heart failure, stroke, and unplanned late revascularization.
What is the main result?
Endothelium-dependent microvascular dysfunction (%ΔCBF-Ach < 50 %) was demonstrated in 51.8 % of the population and endothelium-independent microvascular dysfunction (CFR < 2.5) in 24.5 %. Endothelium-dependent epicardial coronary artery dysfunction (%ΔCAD-Ach < − 20 %) was seen in 25.4 % and endothelium-independent epicardial coronary artery dysfunction (%ΔCSA-NTG < 20 %) in 47.4 %.
Concomitant endothelium-independent and dependent epicardial coronary artery dysfunction was higher in patients with endothelium-dependent microvascular dysfunction than those without (53.5 % vs 40.9 % and 38.4 % vs 11.4 %; P < 0.001). Concomitant endothelium-independent epicardial coronary artery dysfunction (52.6 % vs 45.7 %; P = 0.049) but not endothelium-dependent epicardial coronary artery dysfunction (24.9 % vs 25.6 %; P = 0.873) was seen in patients with endothelium-independent microvascular dysfunction.
The median age was 52 years with 71 % of patients female, traditional cardiovascular risk factors were present in approximately half the population with a median follow-up of 6.3 years.
- MACCE rates were higher in patients with endothelium-dependent microvascular dysfunction compared to those without (19.5 % vs 12 %, p < 0.001), endothelium-independent microvascular dysfunction compared to those without (; 22.2 % vs 13.8 %, p = 0.001) and endothelium-dependent epicardial coronary artery dysfunction compared to those without (19.7 % vs 14.6 %, p = 0.038). There were no differences in MACCE in patients with and without endothelium-independent epicardial coronary artery dysfunction (16.4 % vs 15.4 %; P = 0.701)
- Following multivariate analysis coronary flow reserve (HR: 0.998, 95 % CI: 0.604-0.957, p = 0.020) and change in coronary blood flow after Ach (HR: 0.998, 95 % CI: 0.996-0.999) were significant predictors of major adverse cardiac and cerebrovascular events.
- Microvascular CVDys was associated with a significantly higher risk for adverse events compared with those with normal microvascular function (p < 0.001).
Critical reading and the relevance for clinical practice
In this large single centre registry, investigators demonstrated that, with the exception of endothelium independent epicardial coronary artery dysfunction, CVDys diagnosed by interventional functional assessment is correlated with adverse cardiac and cerebrovascular events. The diagnostic process requires 4 steps with 3 vasoactive intracoronary drugs and a dedicated doppler wire however can accurately differentiate each CVDys phenotype.
This majority of patients with angina and no significant stenosis in the epicardial vessels undergoing CRT in this study, 76.3 %, had microvascular dysfunction. This study was carried out in a high volume CRT centre, however, this real-world retrospective data add more evidence towards the benefit of performing functional tests in patients with angina or signs of stable ischemia. There is presently no dedicated treatment for microvascular disease, however the CorMicA trial2 demonstrated improved outcomes with targeted treatment based on CVDsy phenotype.
Coronary flow reserve was measured as a surrogate of endothelium-independent microvascular dysfunction; however as it provides a global assessment of the coronary circulation, it can be reduced in the presence of epicardial disease. Other more selective indices, as the index of microcirculatory resistance (iMR), the hyperaemic microcirculatory resistance (hMR) and the microvascular resistance reserve (MRR), are widely studied and commercially available. Of note, recent trial has demonstrated very high specificity of treadmill stress test in the diagnosis of microvascular CVDys in patients with coronary ischemia/angina3. Another categorization of coronary artery disease has been also proposed and based on 4 endotypes including obstructive disease.
The exclusion of patients with obstructive coronary disease, myocardial bridge and severe spasm after Ach may underestimated the prevalence of CVDys and diluted the real rates of major adverse events in CVDys patients.
A number of important limitations exist with regard to this study including the current challenges obtaining the doppler wire used for CRT. Assessment of the population included in the trial began in 1997 and there have been significant advances in diagnostics since then with evolution of CRT from a niche assessment in selected centres to a guideline recommendation.
Overall, this data supports the high prevalence and the clinical significance of CVD in patients with ANOCA. Microvascular and endothelium-dependent epicardial CVD lead to adverse events and more research towards therapeutic strategies is warranted.
References
- Kanaji Y, Ahmad A, Singh Sara JD, Ozcan I, Akhiyat N, Prasad A, Raphael CE, Kakuta T, Lerman LO, Lerman A. Coronary Vasomotor Dysfunction Is Associated With Cardiovascular Events in Patients With Nonobstructive Coronary Artery Disease. JACC Cardiovasc Interv. 2024 Feb 26;17(4):474-487. doi: 10.1016/j.jcin.2023.11.039.
- Ford TJ, Stanley B, Good R, Rocchiccioli P, McEntegart M, Watkins S, Eteiba H, Shaukat A, Lindsay M, Robertson K, Hood S, McGeoch R, McDade R, Yii E, Sidik N, McCartney P, Corcoran D, Collison D, Rush C, McConnachie A, Touyz RM, Oldroyd KG, Berry C. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina: The CorMicA Trial. J Am Coll Cardiol. 2018 Dec 11;72(23 Pt A):2841-2855. doi: 10.1016/j.jacc.2018.09.006.
- Sinha A, Dutta U, Demir OM, De Silva K, Ellis H, Belford S, Ogden M, Li Kam Wa M, Morgan HP, Shah AM, Chiribiri A, Webb AJ, Marber M, Rahman H, Perera D. Rethinking False Positive Exercise Electrocardiographic Stress Tests by Assessing Coronary Microvascular Function. J Am Coll Cardiol. 2024 Jan 16;83(2):291-299. doi: 10.1016/j.jacc.2023.10.034.


No comments yet!