Intravascular imaging vs angiography guided complex PCI: 5-year outcomes from a randomised trial
Selected in JACC by A. McInerney , N. Gonzalo
The RENOVATE-COMPLEX-PCI 5-year outcomes confirm the long-term durability of benefits seen with intracoronary imaging over angiography guided PCI in complex lesions.
References
Authors
Joo Myung Lee, Onyou Kim, Young Bin Song, Jong-Young Lee, Seung-Jae Lee, Sang Yeub Lee, Sang Min Kim, Kyeong Ho Yun, Jae Young Cho, Chan Joon Kim, Hyo-Suk Ahn, Chang-Wook Nam, Hyuck-Jun Yoon, Yong Hwan Park, Wang Soo Lee, Jin-Ok Jeong, Pil Sang Song, Joon-Hyung Doh, Sang-Ho Jo, Chang-Hwan Yoon, Min Gyu Kang, Jin-Sin Koh, Kwan Yong Lee, Young-Hyo Lim, Yun-Hyeong Cho, Jin-Man Cho, Woo Jin Jang, Kook-Jin Chun, Ki Hong Choi, Taek Kyu Park, Jeong Hoon Yang, Seung-Hyuk Choi, Hyeon-Cheol Gwon, and Joo-Yong Hahn
Reference
10.1016/j.jacc.2026.01.035
Published
4 March 2026
Link
Read the abstractReviewers


Our Comment
RENOVATE-COMPLEX-PCI 5 year results
Why this study – the rationale/objective?
Intracoronary imaging is known to provide additional information beyond that available from angiography alone to guide and optimise percutaneous coronary intervention (PCI).
Multiple studies and large meta-analyses have demonstrated improved outcomes when PCI is guided by intracoronary imaging compared to angiographic guidance1. Most studies, however, have reported short to mid-term outcomes only 1-3.
Whether the immediate and short term benefits of intracoronary imaging in complex lesions translates to durable outcomes at long term follow-up has not been demonstrated.
The 5-year follow up of the RENOVATE-COMPLEX-PCI aimed to explore the durability of the benefits of intracoronary imaging guided complex PCI4.
How was it executed – the methodology?
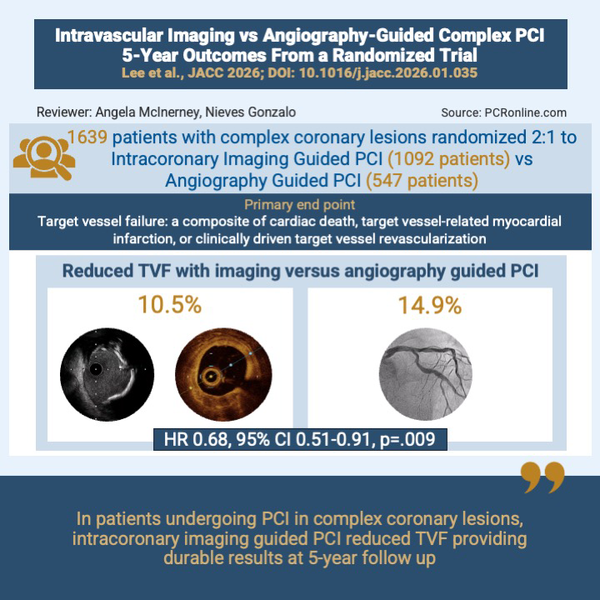
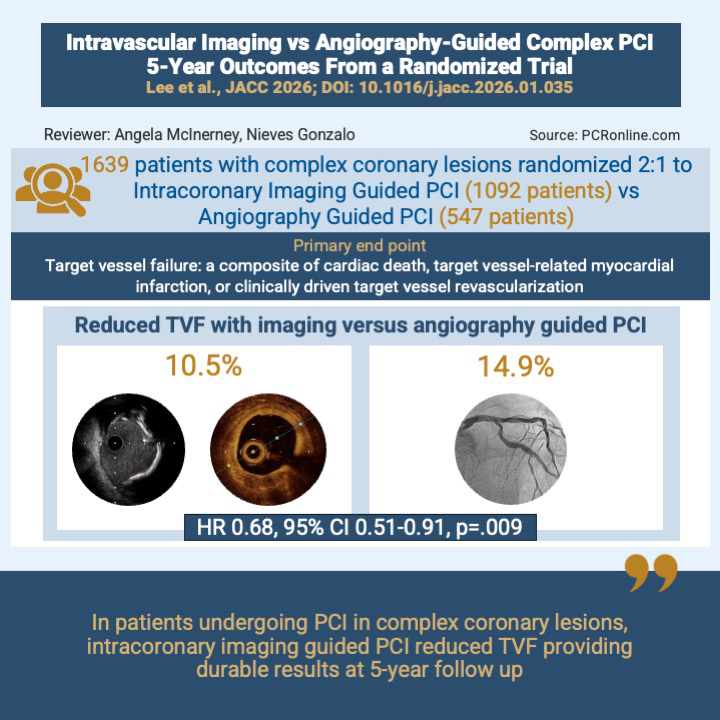
This was a multicentre, open labelled randomised controlled trial performed across 20 hospitals in South Korea. Patients undergoing complex PCI were eligible for enrolment. Randomisation was on a 2:1 ratio to intracoronary imaging or angiography guided PCI.
Complex PCI was defined as true bifurcations, chronic total occlusions, unprotected left main stem, long lesions (requiring > 38 mm of stent), multivessel PCI, ≥ 3 stents, instent restenosis, severe calcification and aorto-ostial lesions.
The choice of intracoronary imaging modality (OCT or IVUS) was at the operators discretion.
In patients assigned to the intracoronary imaging group, this could be performed at any point during the procedure, but was mandated following stent implantation to guide optimisation.
Primary end point
The primary endpoint was target vessel failure (TVF): a composite of cardiac death, target vessel-related myocardial infarction (TV-MI), or clinically driven target vessel revascularisation (CD-TVR).
Secondary end points
Secondary endpoints included:
- Individual components of the primary endpoint
- Target vessel failure without procedure-related myocardial infarction
- A composite of cardiac death or target vessel–related myocardial infarction
- Definite stent thrombosis
- Contrast-induced nephropathy
- Bleeding
Exploratory endpoint
An exploratory endpoint comparing the results of “optimised” versus “non-optimised” intracoronary imaging guided PCI was performed.
Optimised imaging guided PCI was defined as:
< 10 % stenosis visually by angiography AND stent expansion
Non-left main lesions:
Minimum stent area (MSA) > 80 % of the average reference lumen area or MSA > 5.5 mm2 by IVUS or > 4.5 mm2 by OCT
Left main lesions:
MSA > 7 mm2 for distal left main and > 8 mm2 for proximal left main artery by IVUS
Stent apposition:
No major malapposition of ≥ 0.4 mm with longitudinal extension > 1 mm
Edge dissection:
No major edge dissection defined as dissection within 5 mm of the proximal or distal stent edges, extending to the media with ≥ 60° of the circumference of the vessel and extending for ≥ 3 mm in length
What is the main result?
Two-year results of the RENOVATE-COMPLEX-PCI study have been previously reported5. The current study reports the long-term follow-up of these patients (median follow up 5.3 years)4. 1,639 patients were randomised: 1,092 imaging-guided, 547 angiography-guided PCI. Approximately half the enrolled patients presented with acute coronary syndromes. The most common definition of complexity were long lesions (≥ 38 mm stenting required), followed by true bifurcations (~ 22 %) and CTO (~ 20 %). Approximately 30 % of patients had ≥ 3 complex characteristics. IVUS was the most commonly used intravascular imaging technique (~ 75 %) with OCT being used in ~ 25 %. Most patients (~ 75 %) in the intracoronary imaging arm had both pre- and post-stent imaging performed (data in supplementary appendix). Procedural success in both arms was high and not different between groups.
The primary endpoint of TVF occurred in 10.5 % in the intravascular imaging group versus 14.9 % in the angiography-guided group (HR, 0.68; 95 % CI 0.51 to 0.91; p = 0.009). The primary endpoint was primarily driven by a reduction in the composite of cardiac death or TVMI in the intracoronary imaging group (7.6 % vs 10.7 %; HR: 0.68; 95 % CI: 0.48-0.96; P = 0.029). TVR and TLR were not different between groups, however edge restenosis was numerically lower in the intracoronary imaging guided group (8 of 35 TLR (22.9 %) vs. 10 of 25 TLR (40 %) in the angiography-guided group).
A landmark analysis at 2 years demonstrated the predominant benefit of intracoronary imaging guidance on TVF occurred in the first 2 years (7.4 % vs. 10.9 %; HR: 0.69; 95 % CI: 0.51-0.93; p = 0.013), with event rates remaining low after 2 years but not statistically different between groups (3.4 % vs. 4.5 %; HR 0.72; 95 % CI: 0.40-1.29; p = 0.267). No late catch up phenomena was noted in the intracoronary imaging group.
Patients with an “optimised result” in the intracoronary imaging arm had significantly lower incidence of the primary end point compared to “non-optimised”, but imaged stents and compared to angiography guided stenting (9.1 % vs 11.7 % vs 14.9 %, overall log-rank p = 0.017).
Critical reading and the relevance for clinical practice:
This randomised controlled trial represents the longest available follow for patients with various complex lesions randomized to intracoronary imaging versus angiography guided PCI. This demonstrates for the first time, that intracoronary imaging provides improved and importantly, durable results compared to angiography guided PCI at long-term follow-up.
The study has a number of strengths which are well outlined in the accompanying editorial published with the original manuscript in JACC6, including the large number of patients randomised with robust methodology and clearly defined, clinically relevant end points.
The finding of durable results out to five years strengthens the case for intracoronary imaging to guide PCI in these complex lesion subsets. Although not powered to assess the impact of imaging on each lesion subtype included, long lesions and CTO seemed to derive particular benefit from intracoronary imaging with a tendency to benefit for unprotected left main stem and calcified lesions. Although p values for these latter two lesion subsets do not reach statistical significance, this may be related to smaller numbers of these particular lesion subsets being included in the study.
The landmark analysis provides important insights into the benefits of intracoronary imaging. The main benefit is seen within the periprocedural and early post procedure time period. Beyond 2 years, events continue to accrue but at a low rate in both groups without statistically significant differences between treatment arms. Furthermore the exploratory analysis of “optimised” versus “non-optimised” imaging guided outcomes is insightful. The reduced incidence of TVF in the imaging arm for those who had ‘optimised’ stenting results further reinforces the need to act on the imaging findings rather than just simply performing imaging.
The limitations of this study are well outlined by the authors and include the fact that it was performed entirely in South Korea and so extrapolation to other populations may be difficult. However, other studies performed in different geographical locations have also demonstrated similar benefits with the use of intracoronary imaging in these complex lesions, albeit with shorter follow up2, 3, 7. The results of the recent IVUS-CHIP study are somewhat at odds to the RENOVATE-COMPLEX-PCI study with a similar complex patient cohort but a short follow up (median 19 months)8. Whether longer term follow up in the IVUS-CHIP trial demonstrates divergence in outcomes between imaging and angiography guidance remains to be seen.
Conclusion
In conclusion, the RENOVATE-COMPLEX-PCI 5 year results provide the longest data to date demonstrating the benefits of intracoronary imaging over angiography guidance for complex lesions. As outlined in the accompanying editorial to the trial, these data encourages us to “optimise today for lasting outcomes tomorrow”6.
References
- Stone GW, Christiansen EH, Ali ZA, Andreasen LN, Maehara A, Ahmad Y, et al. Intravascular imaging-guided coronary drug-eluting stent implantation: an updated network meta-analysis. Lancet. 2024;403(10429):824-37.
- Gao XF, Ge Z, Kong XQ, Kan J, Han L, Lu S, et al. 3-Year Outcomes of the ULTIMATE Trial Comparing Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation. JACC Cardiovasc Interv. 2021;14(3):247-57.
- Holm NR, Andreasen LN, Neghabat O, Laanmets P, Kumsars I, Bennett J, et al. OCT or Angiography Guidance for PCI in Complex Bifurcation Lesions. N Engl J Med. 2023;389(16):1477-87.
- Lee JM, Kim O, Song YB, Lee JY, Lee SJ, Lee SY, et al. Intravascular Imaging- vs Angiography-Guided Complex PCI: 5-Year Outcomes From a Randomized Trial. J Am Coll Cardiol. 2026.
- Lee JM, Choi KH, Song YB, Lee JY, Lee SJ, Lee SY, et al. Intravascular Imaging-Guided or Angiography-Guided Complex PCI. N Engl J Med. 2023;388(18):1668-79.
- Gonzalo N, McInerney A. Intravascular Imaging to Guide Percutaneous Coronary Intervention: Optimize Today for Lasting Outcomes Tomorrow. J Am Coll Cardiol. 2026.
- Hong SJ, Mintz GS, Ahn CM, Kim JS, Kim BK, Ko YG, et al. Effect of Intravascular Ultrasound-Guided Drug-Eluting Stent Implantation: 5-Year Follow-Up of the IVUS-XPL Randomized Trial. JACC Cardiovasc Interv. 2020;13(1):62-71.
- Diletti R, Daemen J, Faurie B, Barbierato M, Tchetche D, Hovasse T, et al. Intravascular Ultrasound-Guided or Angiography-Guided Complex High-Risk PCI. N Engl J Med. 2026.
No comments yet!