NOBLE trial: 10-year outcomes of PCI vs CABG in left main disease
Selected in The Lancet by R. Sava
Long-term evidence comparing PCI and CABG for unprotected left main coronary disease has been limited and sometimes conflicting. The 10-year results from the NOBLE trial now provide important clarity on all-cause mortality outcomes with both revascularisation strategies.
References
Authors
Emil Nielsen Holck, Niels R Holm, Prof David Hildick-Smith, M Mitchell Lindsay, Prof Mark S Spence, Prof Andrejs Erglis, Prof Ian B A Menown, Terje Steigen, Lone Juul Hune Mogensen, MStat, Ivy Susanne Modrau, Dr Med, Matti Niemelä, PhDk ∙ Prof Jens F Lassen, PhDl ∙ Prof Keith Oldroyd, MDe ∙ Prof Peteris Stradins, Simon J Walsh, Petter C Endresen, Thor Trovik, Prof Ole Fröbert, Alastair N J Graham, Vesa Anttila, Uday Trivedi, Leif Thuesen, Prof Evald H Christiansen
Reference
Volume 407, Issue 10536, p1374-1382, April 04, 2026
Published
April 04, 2026
Link
Read the abstractReviewer

My Comment
Why this study – the rationale/objective?
Long-term data regarding outcomes of patients treated by percutaneous coronary intervention (PCI) for left main (LM) coronary artery disease using modern drug eluting stents are lacking.
Data regarding mid- and long-term all-cause mortality are conflicting: while older studies comparing PCI with first generation stents versus coronary artery bypass graft (CABG) surgery showed similar all-cause mortality rates at 52 and 10 years3, PCI with second generation drug-eluting stents (DES) in the EXCEL trial was associated with higher 5-year mortality4.
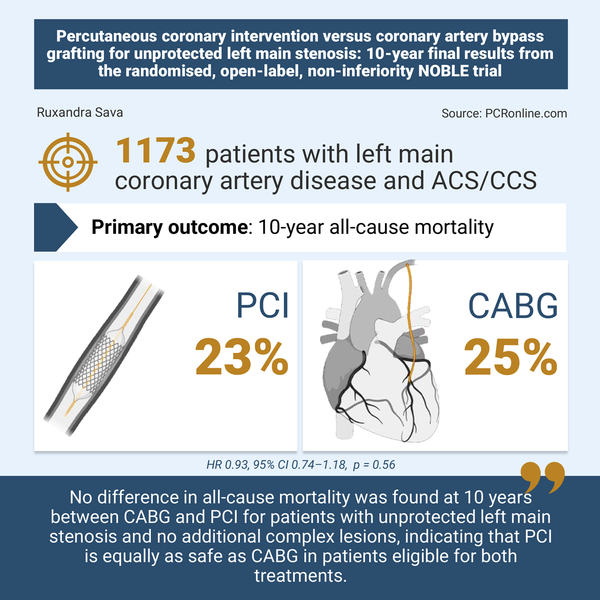
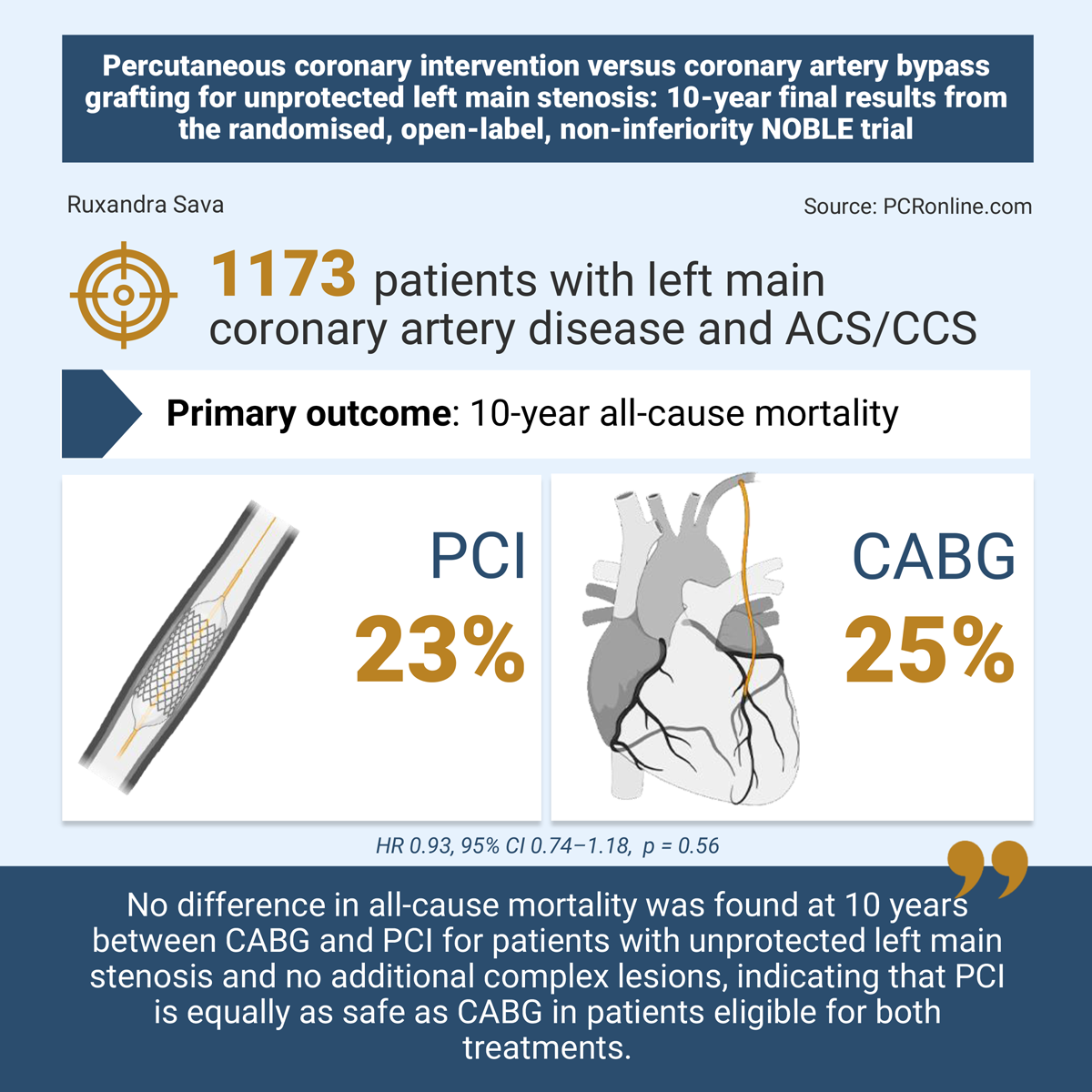
This 10-year follow-up of the NOBLE randomised trial attempted to bridge this gap in knowledge, by comparing all-cause mortality between PCI with second generation DES versus CABG for the treatment of unprotected LM stenosis.
How was it executed – the methodology?
The Nordic–Baltic–British Left main rEvascularization study (NOBLE)1 was a prospective, randomised, open-label and non-inferiority trial which enrolled patients at 36 hospitals in Denmark, Estonia, Finland, Germany, Latvia, Lithuania, Norway, Sweden, and the UK between 2008 and 2015.
Patients presenting with a chronic or an acute coronary syndrome (unstable angina or NSTEMI) and with a left-main stenosis of at least 50 % or an FFR <= 0.80, judged eligible for both PCI and CABG, could be included in the study.
Exclusion criteria included STEMI, an additional complex lesion or at least three other non-complex lesions, and prior CABG.
For the purpose of this analysis, vital status was assessed using a medical record audit or an active health insurance at the time of the audit.
What is the main result?
Out of the 1,184 patients included in the ITT population (592 in each group), 10-year survival data was available for 1,173 patients. The mean age was 66.2 years in both the PCI and the CABG group. Women represented a minority of trial participants (256 patients, 22 %). EUROSCORE-2 scores (2 in both groups), the prevalence of distal left main disease (81 % in both groups, p=0.77) and clinical presentation (CCS: 82 % in the PCI arm, 83 % in the CABG arm; ACS 18 % and 17 %, respectively; p = 0.66) were similar between groups.
At 10 years, there was no difference between the rate of all-cause mortality in the PCI and the CABG group: 136 patients (23 %) versus 145 patients (25 %), hazard ratio 0.93, 95 % CI 0.74–1.18, p = 0.56.
Critical reading and the relevance for clinical practice:
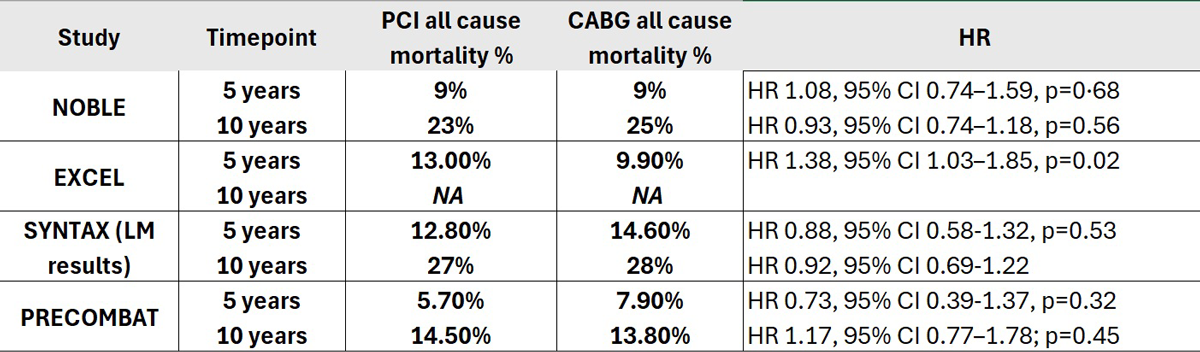
This 10-year analysis of patients with significant LM disease enrolled in the NOBLE trial and randomised to PCI or CABG showed similar all-cause mortality with both treatment strategies. These results are consistent with prior 5-year results (9 % in both groups, HR 1.06, 95 % CI 0.73–1.55, p = 0.76). However, they differ from those reported by the only other randomised trial of LM revascularization using contemporary drug-eluting stents, as all-cause mortality in EXCEL4 was higher in the PCI arm (Table). To explore a potential late catch-up of mortality in the PCI arm, the investigators of NOBLE conducted a time-restricted landmark analysis between 5-10 years, which showed similar all-cause mortality rates (15 % in the PCI group, 17 % in the CABG group, HR 0.86, 95 % CI 0.64–1.16, p = 0.32). Moreover, these findings are also consistent with those of the SYNTAX2,3 and PRECOMBAT5,6 trials, in which PCI with first generation drug-eluting stents was associated with mortality rates broadly comparable to CABG (Table).
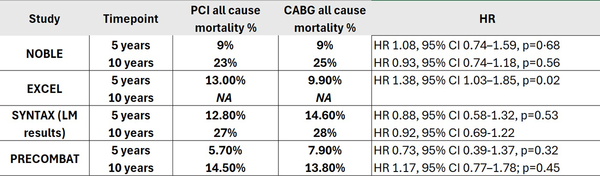
Table showing all-cause mortality rates at 5 and 10 years in the four main randomised trials comparing outcomes following PCI or CABG. HR, hazard ratio.
Whether patients with an acute coronary syndrome (ACS) related to a LM lesion benefit more from PCI than from CABG remains a matter of debate. An individual patient data pooled analysis of the four randomised clinical trials SYNTAX, PRECOMBAT, EXCEL and NOBEL found no significant difference between rates of all-cause mortality at 5 years between PCI and CABG, irrespective of clinical presentation, and no significant interaction between treatment strategy and clinical presentation5. Similar findings were observed in the real-world DELTA registry, in which ACS patients with LM disease treated with PCI or CABG had similar 4-year mortality rates7.
In the present study, the hazard ratio for all-cause mortality favored PCI in patients presenting with an ACS (HR 0.57, 95 % CI 0.32–0.99), whereas no significant difference was observed in the chronic coronary syndrome subgroup (HR 1.04, 95 % CI 0.80–1.34), with a borderline interaction term (p = 0.049). The longer median time to revascularisation in the CABG arm compared with the PCI arm (6 vs 1 day) may partially account for this finding, as earlier revasculariation is associated with improved outcomes in ACS. However, given the post-hoc nature of this analysis, the limited power for subgroup comparisons and the small proportion of patients presenting with an ACS (18 % and 17 % in the PCI and CABG group, respectively), these findings should be interpreted with caution. Overall, these results support the view that both PCI and CABG remain reasonable revasculariisation strategies for selected patients presenting with an ACS due to a LM lesion.
Interestingly, the present analysis did not find any interaction between all-cause mortality and the SYNTAX score. However, this evaluation is limited by enrollment of low numbers of patients with high SYNTAX scores (46 and 56 patients treated with PCI and CABG, respectively), with most patients having either low (297 and 316, respectively) or intermediate (249 and 220, respectively) SYNTAX scores. Consequently, the study is likely underpowered to detect effect modification across SYNTAX categories. The SYNTAX score remains a widely used and validated tool for assessing anatomical complexity, although it should be interpreted alongside other anatomical and clinical factors when guiding revascularisation strategy.
While performance of intravascular imaging was not pre-specified in the study protocol, 72 % of the patients treated by PCI benefited from post-PCI IVUS assessment8. Even in the absence of predefined stent optimisation criteria, at 10 years all-cause mortality was numerically higher in patients without a final IVUS run (31 % versus 20 %). For context, the dedicated NOBLE IVUS sub-study showed no difference in the rate of MACCE at 5 years, however LM target lesion revascularisation was reduced in the IVUS group (5.1 % vs 11.6 %, p = 0.01).
A number of limitations need to be acknowledged when interpreting the general findings of this study. While all-cause mortality was a pre-specified secondary endpoint, the study was not powered to detect differences in mortality. However, Bayesian analyses incorporating informative priors support the conclusion of no meaningful difference between the PCI and CABG groups. Moreover, any mechanistic interpretation is hindered by the absence of secondary endpoints such as myocardial infarction, stroke, repeat revascularisation, and cause of death. Additional trial weaknesses include lack of data regarding adherence to medical therapy and current advances in guideline-directed medical therapy. Finally, these findings do not apply to patients presenting with a significant LM disease and other additional complex lesions, neither to patients presenting with an ST elevation myocardial infarction, as all such patients were excluded from the study.
Overall, these findings support PCI and CABG as reasonable revascularisation strategies for selected patients with significant LM disease, including those presenting with ACS. Treatment selection should be guided by careful disease phenotyping, with anatomical complexity beyond the SYNTAX score playing a central role, alongside clinical factors. Shared decision-making, with clear discussion of the risks and benefits of each approach, remains essential.
References
- Holck EN, Holm NR, Hildick-Smith D, Lindsay MM, Spence MS, Erglis A, et al. Percutaneous coronary intervention versus coronary artery bypass grafting for unprotected left main stenosis: 10-year final results from the randomised, open-label, non-inferiority NOBLE trial. The Lancet. 2026 Apr 4;407(10536):1374–82. doi: 10.1016/S0140-6736(26)00205-9 PubMed PMID: 41936368.
- Morice MC, Serruys PW, Kappetein AP, Feldman TE, Ståhle E, Colombo A, et al. Five-year outcomes in patients with left main disease treated with either percutaneous coronary intervention or coronary artery bypass grafting in the synergy between percutaneous coronary intervention with taxus and cardiac surgery trial. Circulation. 2014 Jun 10;129(23):2388–94. doi: 10.1161/CIRCULATIONAHA.113.006689 PubMed PMID: 24700706.
- Thuijs DJFM, Kappetein AP, Serruys PW, Mohr FW, Morice MC, Mack MJ, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. The Lancet. 2019 Oct 12;394(10206):1325–34. doi: 10.1016/S0140-6736(19)31997-X PubMed PMID: 31488373.
- Five-Year Outcomes after PCI or CABG for Left Main Coronary Disease | NEJM. New England Journal of Medicine. Available from: https://www.nejm.org/doi/full/10.1056/NEJMoa1909406
- Gaba P, Christiansen EH, Nielsen PH, Murphy SA, O’Gara PT, Smith PK, et al. Percutaneous Coronary Intervention vs Coronary Artery Bypass Graft Surgery for Left Main Disease in Patients With and Without Acute Coronary Syndromes: A Pooled Analysis of 4 Randomized Clinical Trials. JAMA Cardiol. 2023 Jul 1;8(7):631–9. doi: 10.1001/jamacardio.2023.1177
- Park DW, Ahn JM, Park H, Yun SC, Kang DY, Lee PH, et al. Ten-Year Outcomes After Drug-Eluting Stents Versus Coronary Artery Bypass Grafting for Left Main Coronary Disease. Circulation. 2020 May 5;141(18):1437–46. doi: 10.1161/CIRCULATIONAHA.120.046039
- Pyxaras S, Hunziker L, Chieffo A, Meliga E, Latib A, Park SJ, et al. Long-term clinical outcomes after percutaneous coronary intervention versus coronary artery bypass grafting for acute coronary syndrome from the DELTA registry: a multicentre registry evaluating percutaneous coronary intervention versus coronary artery bypass grafting for left main treatment. Available from: https://eurointervention.pcronline.com/article/long-term-clinical-outcomes-after-percutaneous-coronary-intervention-versus-coronary-artery-bypass-grafting-for-acute-coronary-syndrome-from-the-delta-registry-a-multicentre-registry-evaluating-percutaneous-coronary-intervention-versus-coronary-artery-bypass-grafting-for-left-main-treatment?utm_source=chatgpt.com doi: 10.4244/EIJV12I5A102
- Ladwiniec A, Walsh S, Holm N, Hanratty C, Mäkikallio T, Kellerth T, et al. Intravascular ultrasound to guide left main stem intervention: a NOBLE trial substudy [Internet]. [cited 2026 Apr 12]. Available from: https://eurointervention.pcronline.com/article/intravascular-ultrasound-to-guide-left-main-stem-intervention-a-sub-study-of-the-noble-trial doi: 10.4244/EIJ-D-19-01003.
No comments yet!