Computed tomography versus near-infrared spectroscopy for the assessment of coronary atherosclerosis
Selected in EuroIntervention Journal by C. Said , N. Ryan
NIRS-IVUS offers precise assessment of coronary artery pathology but is invasive and limited in scope, while CCTA is emerging as a non-invasive alternative for comprehensive plaque evaluation.
References
Authors
Anantharaman Ramasamy, Ramya Parasa, Hessam Sokooti, Xiaotong Zhang, Ibrahim Halil Tanboga, Pieter Kitslaar, Alexander Broersen, Krishnaraj S. Rathod, Rajiv Amersey, Ajay Jain, Mick Ozkor, Johan H.C. Reiber, Jouke Dijkstra, Patrick W. Serruys, James C. Moon, Anthony Mathur, Ryo Torii, Francesca Pugliese, Andreas Baumbach, Christos V. Bourantas
Reference
DOI: 10.4244/EIJ-D-24-00096
Published
December 2, 2024
Link
Read the abstractReviewers

Our Comment
Designed by Christian F Said. Source: PCRonline
Why this study – the rationale/objective?
Intravascular imaging with near-infrared spectroscopy-intravascular ultrasound (NIRS-IVUS) provides accurate assessment of coronary artery pathology allowing for improved clinical outcomes1-5. NIRS-IVUS however, is invasive and is limited to specific segments of the coronary tree.
Coronary computed tomography angiography (CCTA) is receiving increased attention as a non-invasive alternative for evaluating plaque pathology across the entire coronary tree6,7.
How was it executed – the methodology?
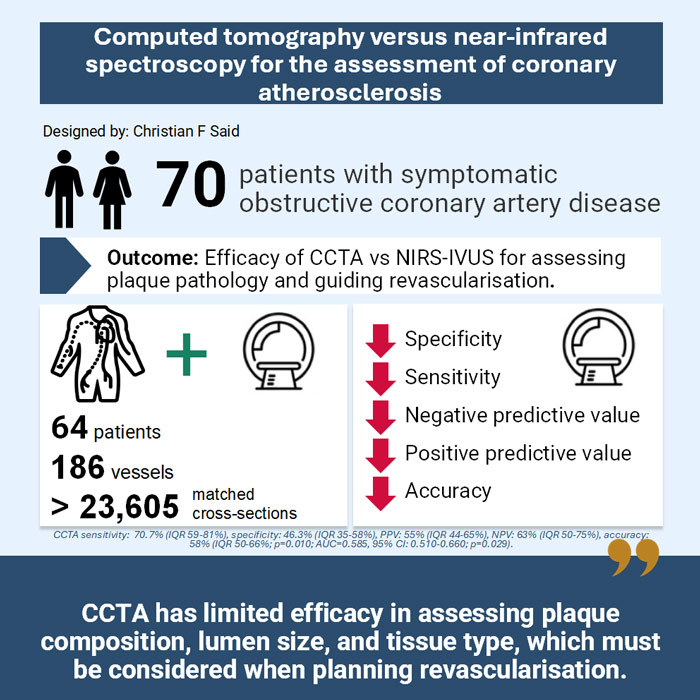
This prospective, single-centered study recruited 70 patients with chronic coronary syndrome and obstructive coronary artery disease on invasive angiography undergoing further assessment (pressure wire or intracoronary imaging) or treatment (PCI). All patients underwent CCTA and multi-vessel NIRS-IVUS imaging followed by clinically indicated treatment.
- The primary endpoint was the efficacy of plaque composition on CCTA in detecting lipid-rich plaque, using NIRS-IVUS as the reference standard.
- Secondary endpoints included the performance of CCTA in evaluating coronary artery pathology in the studied segments and its value in stent sizing using NIRS-IVUS as the reference standard.
- Plaque on NIRS-IVUS was defined as a segment with plaque burden (PB) > 40 % over three consecutive frames. No CCTA PB cutoff exists so receiver operator curves (ROC) analysis was performed on random lesions to identify the optimum PB cutoff that predicted a PB > 40 % on NIRS-IVUS.
What is the main result?
70 predominantly male patients aged 62 ± 9 years old with chronic coronary syndrome and obstructive coronary artery disease on coronary angiography were recruited. After exclusions for poor image quality, 64 patients were included in the final analysis. 50 vessels from 15 patients were randomly selected to define the optimal plaque burden (PB) cutoff for predicting plaques (necrotic core cutoff of > 1 mm3). The primary endpoint was subsequently evaluated in the remaining 49 patients. 136 vessels and 23,000 matched NIRS-IVUS and CCTA cross sections were included in the final analysis.
- Of 75 lipid-rich plaques detected by NIRS-IVUS, CCTA correctly detected 53 lipid-rich plaques but misclassified 44 others as lipid-rich.
- The sensitivity of CCTA was 70.7 % (IQR 59-81 %), specificity was 46.3 % (IQR 35-58 %), PPV was 55 % (IQR 44-65 %), NPV was 63 % (IQR 50-75 %) and accuracy was 58 % (IQR 50-66 %; p = 0.010; AUC = 0.585, 95 % CI: 0.510-0.660; p = 0.029).
- CCTA overestimated lumen, vessel, and plaque dimensions and poorly correlated with NIRS-IVUS for plaque composition.
Critical reading and the relevance for clinical practice
Although CCTA mitigates the invasive risks of NIRS-IVUS assessment of coronary lesions, there remain significant limitations in the use for CCTA for both evaluation of plaque composition and revascularisation planning.
The agreement between CCTA and NIRS-IVUS for assessing plaque composition was limited with CCTA having a moderate accuracy in detecting lipid-rich plaques. CCTA failed to detect fibrotic plaques in some cases resulting in an underestimation of the stent length particularly in fibrotic lesions with diffuse disease.
This study was designed to overcome previous limitations regarding over- and under-estimation of lumen area and plaque burden by CCTA. Despite the trial being carried out using a prospectively designed, specific reconstruction protocol using third generation CT scanners, CCTA demonstrated limited efficacy in assessing vessel size. For instance, for a patient in this study PCI guided by NIRS-IVUS would have resulted in the use a 3.5 mm stent, whereas CCTA guidance would result in a 3.0 mm stent. This under sizing of stents has the potential to impact clinical outcomes in the longer term8-10 and warrants consideration.
A significant limitation of this paper is that there are no established plaque burden (PB) cutoffs for CCTA to define plaques. To address this the authors used receiver operating characteristics curves (ROC) analysis to identify optimal PB cutoffs that predicted a PB ≥ 40 % on NIRS-IVUS. It remains uncertain whether using an alternative PB cutoff to define landing zones on CCTA would have led to different outcomes.
Finally, it is unclear whether these findings can be generalised to other centres with different equipment, CT reconstruction protocols, or patients with acute coronary syndromes.
References
- Schuurman AS, Vroegindewey M, Kardys I, Oemrawsingh RM, Cheng JM, de Boer S, et al. Near-infrared spectroscopy-derived lipid core burden index predicts adverse cardiovascular outcome in patients with coronary artery disease during long-term follow-up. Eur Heart J. 2018;39(4):295-302.
- Torguson R, Shlofmitz E, Mintz GS, Mario CD, Cate TT, Ali ZA, et al. Frequency of Lipid-Rich Coronary Plaques in Stable Angina Pectoris versus Acute Coronary Syndrome (from the Lipid Rich Plaque Study). Am J Cardiol. 2021;158:1-5.
- Demola P, Di Mario C, Torguson R, Ten Cate T, Bambagioni G, Ali Z, et al. Greater plaque burden and cholesterol content may explain an increased incidence of non-culprit events in diabetic patients: a Lipid-Rich Plaque substudy. Eur Heart J Cardiovasc Imaging. 2022;23(8):1098-107.
- Bambagioni G, Di Mario C, Torguson R, Demola P, Ali Z, Singh V, et al. Lipid-rich plaques detected by near-infrared spectroscopy predict coronary events irrespective of age: A Lipid Rich Plaque sub-study. Atherosclerosis. 2021;334:17-22.
- Erlinge D, Maehara A, Ben-Yehuda O, Bøtker HE, Maeng M, Kjøller-Hansen L, et al. Identification of vulnerable plaques and patients by intracoronary near-infrared spectroscopy and ultrasound (PROSPECT II): a prospective natural history study. Lancet. 2021;397(10278):985-95.
- Ferencik M, Mayrhofer T, Bittner DO, Emami H, Puchner SB, Lu MT, et al. Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients With Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial. JAMA Cardiol. 2018;3(2):144-52.
- Shaw LJ, Blankstein R, Bax JJ, Ferencik M, Bittencourt MS, Min JK, et al. Society of Cardiovascular Computed Tomography / North American Society of Cardiovascular Imaging - Expert Consensus Document on Coronary CT Imaging of Atherosclerotic Plaque - JCTT - DOI: 10.1016/j.jcct.2020.11.002
- Cook S, Wenaweser P, Togni M, Billinger M, Morger C, Seiler C, et al. Incomplete stent apposition and very late stent thrombosis after drug-eluting stent implantation. Circulation. 2007;115(18):2426-34.
- Fujii K, Carlier SG, Mintz GS, Yang YM, Moussa I, Weisz G, et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: an intravascular ultrasound study. J Am Coll Cardiol. 2005;45(7):995-8.
- Song HG, Kang SJ, Ahn JM, Kim WJ, Lee JY, Park DW, et al. Intravascular ultrasound assessment of optimal stent area to prevent in-stent restenosis after zotarolimus-, everolimus-, and sirolimus-eluting stent implantation. Catheter Cardiovasc Interv. 2014;83(6):873-8.


No comments yet!