Focal and diffuse coronary artery disease patterns and placebo-controlled angina relief with percutaneous coronary intervention: ORBITA-2
Selected in JACC by A. McInerney
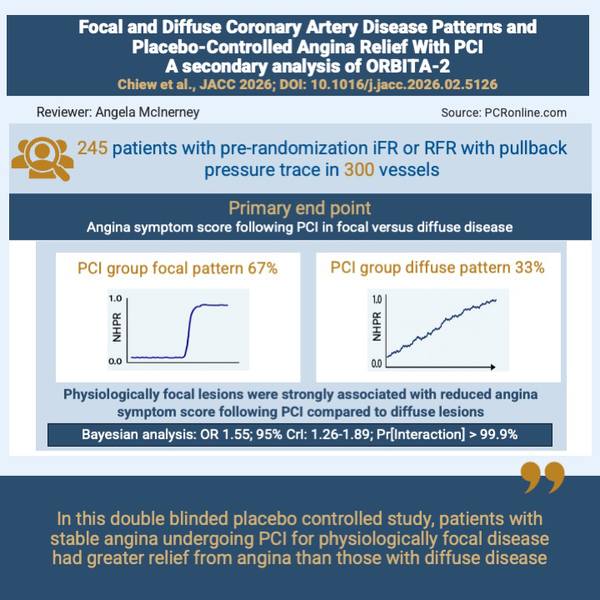
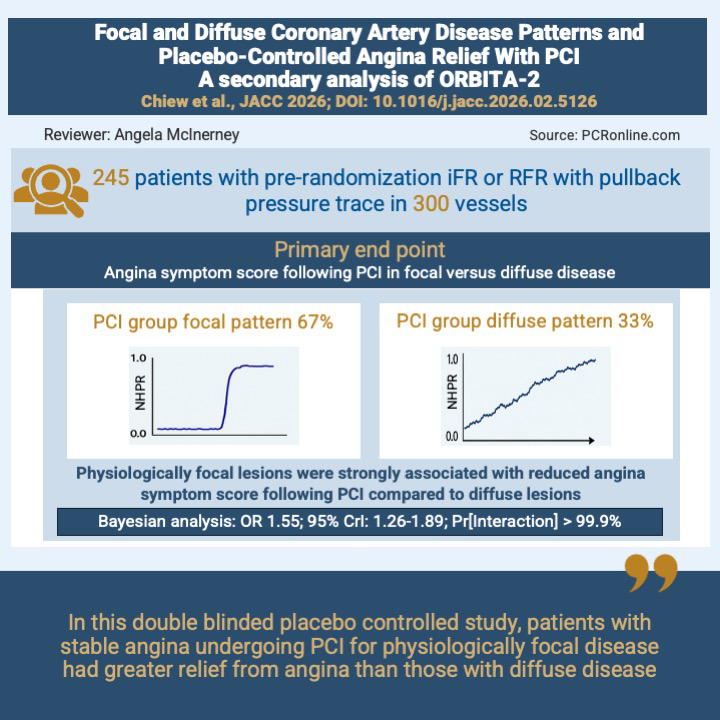
In a secondary analysis of the randomised ORBITA-2 trial, focal coronary artery disease pattern as assessed by non-hyperaemic pressure wire pullback was associated with greater angina relief following PCI than diffuse pattern of disease.
References
Authors
Kayla Chiew, Michael J. Foley, Shayna Chotai, Zahra Naderi, Christopher A. Rajkumar, Fiyyaz Ahmed-Jushuf, Florentina A. Simader, Sharmananthan Ganesananthan, Vaishaanth Nagaraj, Prachur Khandelwal, Adam Hartley, Thomas R. Keeble, Neil Ruparelia, Henry Seligman, Darrel P. Francis, Matthew J. Shun-Shin, and Rasha K. Al-Lamee, the ORBITA-2 Investigators
Reference
DOI: 10.1016/j.jacc.2026.02.5126
Published
22 April 2026
Link
Read the abstractReviewer

My Comment
PCI in physiologically focal versus diffuse disease in stable angina: a secondary analysis of ORBITA-2
Why this study – the rationale/objective?
Many patients with stable angina experience ongoing symptoms despite percutaneous intervention and stenting of the presumed causative lesion. A number of reasons have been suggested for this, including the presence of un-recognised physiologically significant residual disease either within or outside the implanted stent and microcirculatory dysfunction. Disease pattern has also been suggested as a potential cause, but has heretofore not been tested in a randomised placebo-controlled trial.
The current study aims to determine if the pattern of disease (focal versus diffuse) as assessed by non-hyperaemic pressure index pullback traces influences the effectiveness of PCI in reducing symptoms in patients with stable angina.
How was it executed – the methodology?
This was a secondary analysis the ORBITA-2 trial. The ORBITA-2 study was a double blinded, placebo controlled trial which randomised patients with stable angina following discontinuation and wash-out of anti-anginal therapy to PCI versus placebo1. Three hundred and one patients were randomised following angiography and physiological assessment of coronary artery stenosis to either PCI or placebo. The main results of the ORBITA-2 trial demonstrated a significant reduction in angina score in those patients randomised to the PCI arm (mean angina symptom score 2.9 PCI group vs 5.6 in the placebo group (odds ratio, 2.21; 95% confidence interval, 1.41 to 3.47; P<0.001)1.
The current analysis included patients who, as part of their physiological assessment prior to randomisation, underwent non-hyperaemic physiological assessment (NHPR): either instantaneous wave free ratio (iFR) or resting full cycle ratio (RFR), with pullbacks to deduce the pattern of coronary artery disease (focal or diffuse)2. Patients were blinded and were unaware whether they were assigned to the PCI or placebo group as were those performing follow up assessments.
Pullback traces were examined by seven interventional cardiologists and classified as ‘focal’, ‘diffuse’, or ‘mixed’. Disease patterns were analysed as continuous variables, with focal = 1, diffuse = 0, and mixed = 0.5 with the final score for each lesion being the mean score of the 7 assessing cardiologists.
Multiple tests and assessments were performed prior to randomisation and during follow up including daily angina symptoms recorded via the ORBITA app, exercise treadmill test, dobutamine stress echocardiogram, Canadian cardiovascular society angina class, Seattle Angina Questionnaire (SAQ) assessment, Rose questionnaire for angina and the EuroQol Group-5-level (EQ-5D-5L) questionnaire.
Primary endpoint
The primary outcome was the angina symptom score (range 0-79), calculated based on symptoms and anti-anginal medications reported on the ORBITA app. Higher scores indicated worse angina.
Secondary endpoints
Secondary endpoints included:
- Daily angina frequency recorded on the ORBITA-app
- SAQ assessment of angina frequency, physical limitation, angina stability, freedom from angina, symptom stability
- Quality of life assessed with the SAQ and EQ-5D-5L
- Physician-assessed angina severity from the CCS class
- Treadmill exercise time
- Stress echocardiography score.
For analysis of the primary endpoint, a Bayesian Markov longitudinal model was used. This calculated a daily odds ratio of transitioning to a better angina symptoms score of fewer episodes of angina. Adjustment was made for the pre-randomisation non-hyperaemic pressure ratio obtained allowing assessment of the effect of disease pattern alone rather than disease severity on outcomes.
What is the main result?
Physiological pullback traces were available for 245 patients (118 PCI group, 127 placebo group) and 300 vessels. The median age was 65 years and 80% were male. 95% of patients were CCS II or greater.
From the 118 patients included in the PCI group, 79 had focal disease while 39 had diffuse disease. From 127 patients in the placebo arm, 79 had focal disease while 48 had diffuse disease. The median disease pattern score was not different between the PCI and placebo arms (0.71 for both). In lesions with focal disease, the disease pattern score was 0.93 and the pre-randomisation NHPR was 0.63. In lesions with diffuse disease, the disease pattern score was 0.27 and the pre-randomisation NHPR was 0.86.
In those randomised to PCI, a median of 2 stents were implanted with a median stented length of 48 mm and a median stent diameter of 3 mm. Post-PCI physiology demonstrated a NHPR of 0.93. In those with focal disease, the post-PCI NHPR was 0.95 while in the diffuse, it was 0.93.
With regard to the primary endpoint, for patients included in this secondary analysis, there was strong evidence of benefit of PCI in reducing angina symptom score compared to placebo (OR: 1.49; 95% CrI: 1.20-1.82; Pr[Benefit] > 99.9%). When stratified by disease pattern, there was strong evidence of interaction between disease pattern and angina relief with focal disease being associated with greater treatment response compared to diffuse disease (OR: 1.80; 95% CrI: 1.48-2.18; Pr[Benefit] > 99.9%).
Focal disease pattern was also associated with greater treatment response in terms of daily angina episodes, EQ-5D-5L scores and SAQ assessed angina frequency, physical limitation, quality of life and treatment satisfaction. Furthermore, those with focal disease had greater increase in exercise treadmill time (125 s; 95% CrI:67-186; Pr[Interaction] > 99.9%).
Although there was strong evidence of benefit in dobutamine stress echo score with PCI compared to placebo, this did not appear to be affected by disease pattern.
Critical reading and the relevance for clinical practice:
Physiological assessment of epicardial stenosis has predominantly involved the measurement of the physiological impact of a lesion (or lesions) at the most distal point of the vessel. The resulting physiological value obtained was considered in a binary manner to indicate stenting is, or is not, required. In this manner, physiology has acted as a gateway to PCI in patients with angina.
Consideration of the pattern of disease (focal versus diffuse) or using physiology to determine the precise location of physiologically relevant disease within a vessel has not been part of routine assessment. Non-hyperaemic pressure indices, and more recently hyperaemic pullback pressure gradient (PPG), can be used to determine the pattern of disease: focal or diffuse. Furthermore, NHPR co-registration with angiography can locate the point in the vessel where the most pressure loss occurs, paving the way for more precise PCI and prediction of its haemodynamic result3.
This secondary analysis of the ORBITA-2 trial used NHPR and assessed the pattern of disease on pullback of the wire comparing these patterns to outcomes. Patients who had focal lesions treated with PCI experienced a greater response to therapy (PCI) compared with those with diffuse disease. Many clinical outcomes including reduction in angina and improvement in quality of life scores were seen in those with focal disease who underwent PCI compared to diffuse disease. This provides important insights into the efficacy of PCI for angina in different disease patterns and suggests a more tailored approach to the treatment of angina with PCI may be possible.
Previous studies have suggested many patients with angina who undergo PCI still experience symptoms after treatment. A number of reasons have been proposed for this, including the presence of residual physiologically significant disease. In the DEFINE PCI study, 24% of patients had physiologically significant residual disease following PCI and similarly in the TARGET-FFR study, 18.6% of those who underwent FFR guided optimisation, and almost 30% of those in the standard of care arm had physiologically significant residual disease in the treated vessel4,5. Both of these studies demonstrated that unrecognised disease outside of the stented area contributed to the failure to obtain optimal physiological results. This may suggest an element of geographical miss with PCI or indeed that the disease was diffuse in nature and focal stenting was therefore unable to resolve the physiological abnormality. The current study supports this theory that diffuse disease may contribute significantly to the presence of residual angina. In fact a sub-study of the TARGET-FFR study using PPG found similar results suggesting greater relief of angina in focal disease6. The missing element from the current study, however, is the use of this information to guide and plan the PCI with the aim of ‘correcting’ they physiological abnormality. This will be tested in the DEFINE GPS study (NCT 04451044) which has now finished enrolling and is in the follow-up stage. Nonetheless, the current study demonstrates that performing non-hyperaemic pullback assessment prior to PCI gives important insights into the treatment effect of PCI in those with stable angina. The evolution of this finding will be interesting and may change the way in which we guide PCI using physiology although further studies are required to thoroughly assess this possibility.
A number of limitations must be noted. Firstly, the pattern of disease (focal or diffuse) was assessed using visual assessment only and despite multiple interventional cardiologists interpreting each pullback trace, the inter-observer agreement was moderate (Fleiss’ kappa 0.54)2. A more quantitative approach could have been considered whereby “focal” or “diffuse” were defined by a pre-specified change in physiology units over a certain length of the vessel. However, to accurately apply this approach, automatic pullbacks with co-registration to the angiogram would be required. Secondly, despite intracoronary imaging being used in a high proportion of patients, this data was not available for analysis and could have provided greater insights into the PCI performed. Finally, follow-up continued for only 12-weeks and so the long-term impact of PCI for different disease patterns in patients with stable angina cannot be inferred.
Conclusion
In patients with angina and obstructive coronary artery disease by physiological assessment, focal disease pattern resulted in greater response to intervention in terms of angina symptoms, and quality of life.
References
- Rajkumar CA, Foley MJ, Ahmed-Jushuf F, Nowbar AN, Simader FA, Davies JR, et al. A Placebo-Controlled Trial of Percutaneous Coronary Intervention for Stable Angina. N Engl J Med. 2023;389(25):2319-30.
- Chiew K, Foley MJ, Chotai S, Naderi Z, Rajkumar CA, Ahmed-Jushuf F, et al. Focal and Diffuse Coronary Artery Disease Patterns and Placebo-Controlled Angina Relief With Percutaneous Coronary Intervention: ORBITA-2. J Am Coll Cardiol. 2026.
- Nijjer SS, Sen S, Petraco R, Escaned J, Echavarria-Pinto M, Broyd C, et al. Pre-angioplasty instantaneous wave-free ratio pullback provides virtual intervention and predicts hemodynamic outcome for serial lesions and diffuse coronary artery disease. JACC Cardiovasc Interv. 2014;7(12):1386-96.
- Jeremias A, Davies JE, Maehara A, Matsumura M, Schneider J, Tang K, et al. Blinded Physiological Assessment of Residual Ischemia After Successful Angiographic Percutaneous Coronary Intervention: The DEFINE PCI Study. JACC Cardiovasc Interv. 2019;12(20):1991-2001.
- Collison D, Didagelos M, Aetesam-Ur-Rahman M, Copt S, McDade R, McCartney P, et al. Post-stenting fractional flow reserve vs coronary angiography for optimization of percutaneous coronary intervention (TARGET-FFR). Eur Heart J. 2021;42(45):4656-68.
- Collet C, Collison D, Mizukami T, McCartney P, Sonck J, Ford T, et al. Differential Improvement in Angina and Health-Related Quality of Life After PCI in Focal and Diffuse Coronary Artery Disease. JACC Cardiovasc Interv. 2022;15(24):2506-18.
No comments yet!