Impact of device implantation depth on blood flow dynamics after left atrial appendage closure
Selected in EuroIntervention by A. Sticchi
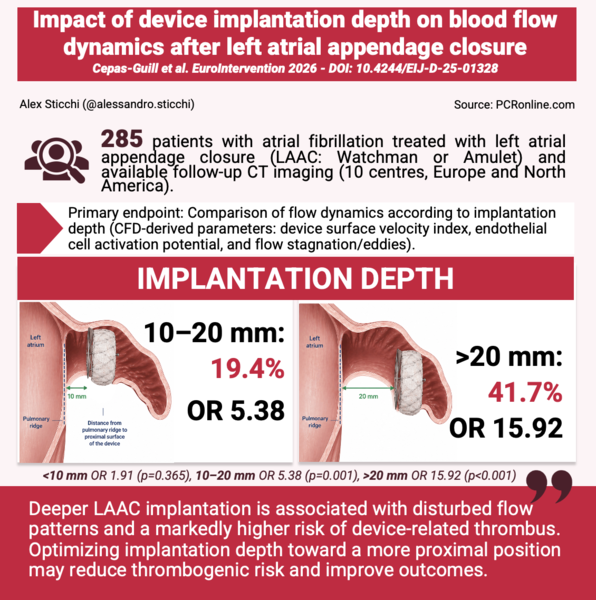
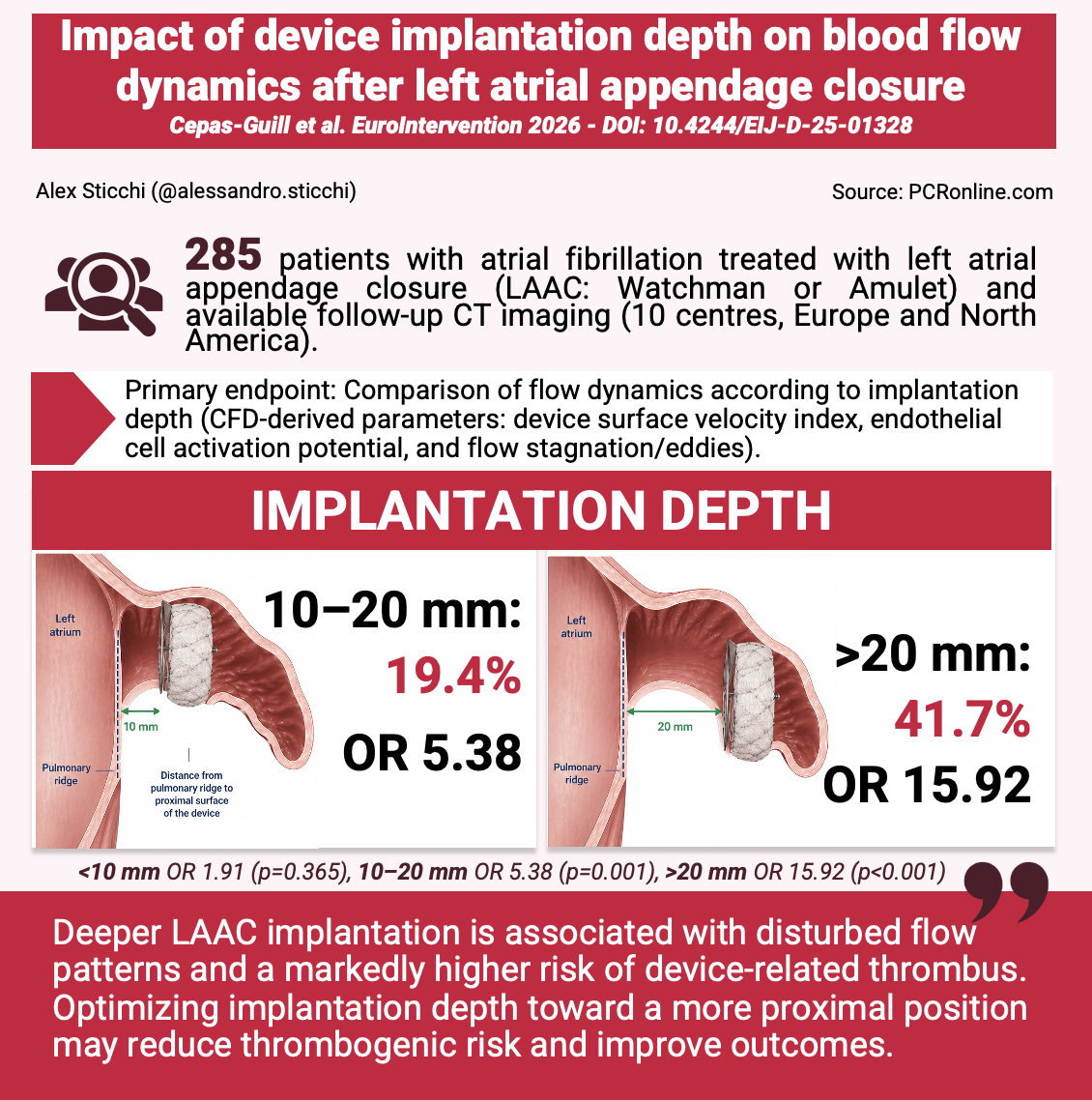
The study aimed to evaluate the impact of LAAC device implantation depth on local flow characteristics and its association with device-related thrombus using patient-specific computational fluid dynamics.
References
Authors
Cepas-Guillén P, Albors C, Mill J, Aminian A, Garot P, De Backer O, Nielsen-Kudsk JE, Iriart X, Barreiro-Perez M, Flores-Umanzor E, Cruz-González I, Arzamendi D, Avvedimento M, Nombela-Franco L, Leduc N, Horvilleur J, Kofoed KF, Korsholm K, Cochet H, Estevez-Loureiro R, Barrouhou M, Lafond A, Millán X, Sanchis L, Rodés-Cabau J, Camara O, Freixa X
Reference
EuroIntervention . 2026 Apr 20;22(8):e444-e454
Published
20 April 2026
Link
Read the abstractReviewer

My Comment
Why this study – the rationale/objective?
Device-related thrombus (DRT) after left atrial appendage closure (LAAC) remains relatively uncommon but clinically meaningful [1]. An updated meta-analysis of 59 studies including 12,845 patients reported a pooled DRT incidence of 2.8%; stroke occurred in 11.5% of patients with DRT versus 2.9% without DRT, and in sensitivity analyses DRT was associated with higher stroke and systemic embolism (OR 4.14 and 4.48, respectively) [2]. Earlier multicentre data had already linked DRT with subsequent adverse clinical events [3]. In the international DRT registry, implantation depth >10 mm from the pulmonary vein limbus was one of the few modifiable predictors of DRT (OR 2.41), while DRT itself was associated with a higher risk of death, ischemic stroke, or systemic embolization (HR 2.37) [4]. Anatomical studies by the same group subsequently showed that pulmonary ridge coverage and more proximal implantation were associated with markedly lower DRT rates, from 27% to 1% in covered versus uncovered pulmonary ridge configurations and from 12.2% to 2.3% in distal versus proximal implants [5,6].
The missing link, however, was mechanistic: why should a deeper implant thrombose more often? The IDEAL-LAAC study was designed to answer exactly this question by testing whether patient-specific computational fluid dynamics (CFD) could demonstrate a reproducible relationship between implantation depth, local haemodynamics, and DRT risk after LAAC [1].
How was it executed? The methodology
This was a multicentre study including 285 patients treated with WATCHMAN or Amplatzer Amulet devices at 10 centres in Europe and North America between January 2019 and October 2023 [1].
The cohort was highly selected: among 1,014 consecutive LAAC patients screened, 490 had follow-up cardiac CT available, and after exclusion of patients with peri-device leak >5 mm, absent transmitral Doppler data, or inadequate CT quality, 285 patients (28.1% of the originally screened population) entered the final CFD analysis [1].
Implant depth was classified as proximal or distal according to device-specific definitions referenced to the pulmonary ridge; for lobe/disc devices, proximal implantation required the disc to be at the pulmonary ridge or <1 mm from it, whereas for single-lobe devices proximal implantation was defined by a distance <10 mm between the ridge and the proximal device surface [1].
Patient-specific left atrial models were reconstructed from post-procedural CT, while boundary conditions incorporated a generic pulmonary venous pressure waveform, patient-specific mitral inflow velocities, and left atrial wall motion [1]. Blood was modelled as a non-Newtonian fluid using the Carreau formulation, five cardiac cycles were simulated for each case, and mean computational time was about 11 hours per patient [1]. The primary endpoint was the difference between proximal and distal implants in three CFD metrics with mechanistic relevance to thrombosis: device surface velocity index (DSVI), endothelial cell activation potential (ECAP), and the presence of eddies or stagnated flow. DRT was adjudicated on contrast-enhanced ECG-gated CT as grade 2 or 3 hypoattenuated thickening [1].
What is the main result?
The study identified a coherent anatomical-haemodynamic-thrombotic gradient [1]. Of the 285 patients, 163 (57.2%) had proximal and 122 (42.8%) distal implants.
Distal implantation was associated with lower device-surface velocity (median DSVI 0.09 vs 0.11 m/s; p=0.002), higher endothelial activation (ECAP 0.90 vs 0.75; p=0.003), and a much greater prevalence of eddies and/or stagnated flow (74.6% vs 40.5%; p<0.001) [1].
Overall DRT incidence was 10.2% (29/285), but risk increased steeply with implant depth: 4.3% for proximal implants, 7.9% for distal implants <10 mm, 19.4% for implants 10-20 mm, and 41.7% for implants >20 mm [1].
Patients with DRT had significantly higher ECAP values (1.10 vs 0.80; p=0.020), and 96.6% of them showed eddies or stagnated flow [1].
In univariable analysis, implantation depth of 10-20 mm and >20 mm carried ORs of 5.38 and 15.92, respectively; ECAP per 0.1 increase had an OR of 1.59, and eddies/stagnated flow an OR of 27.6 [1].
A composite CFD-based score improved discrimination for DRT compared with implant depth alone (AUC 0.81 vs 0.71), and no patient in the low-risk category developed DRT [1].
Critical reading and the relevance for clinical practice:
This is the largest multicentre CFD study performed in LAAC so far and it provides a convincing mechanistic explanation for a clinically familiar observation: deep implants thrombose more often because they generate lower velocities, greater oscillatory shear, and larger recirculation zones near the device surface [1].
Its biological plausibility is reinforced by convergent external evidence. In a 38-patient case-control CFD study, DRT was likewise associated with lower time-averaged wall shear stress (1.76±1.24 vs 2.90±2.70 Pa), higher oscillatory shear index (0.19±0.11 vs 0.17±0.11), and higher ECAP (0.23±0.58 vs 0.17±0.30 Pa-1; p<0.001 for all) [7].
Likewise, the present signal is directionally consistent with prior anatomy-driven series showing DRT rates of 1% versus 27% according to pulmonary ridge coverage [5], and 2.3% versus 12.2% according to proximal versus distal implantation in a 1,317-patient multicentre registry, where distal implant remained independently predictive of DRT (HR 5.92) [6]. Taken together, these studies strongly support a practical procedural message: operators should aim for the most proximal, pulmonary-ridge-covering implant that remains anatomically stable and safe [5,6].
However, translation into routine clinical decision-making still requires caution.
- First, the DRT rate observed here (10.2%) is approximately 3.6-fold higher than the 2.8% pooled incidence reported in the largest meta-analysis and above the roughly 3%-5% range usually quoted in contemporary reviews and consensus documents, suggesting case enrichment and limiting direct extrapolation to an unselected LAAC population [2,11,12].
- Second, only 285 of 1,014 screened patients (28.1%) were ultimately analysed, and only 29 DRT events informed the score, leaving a clear risk of overfitting [1].
- Third, the CFD score was benchmarked mainly against implant depth, not against a full clinical-procedural model; by contrast, the international DRT registry showed that hypercoagulability disorder (OR 17.50), pericardial effusion (OR 13.45), renal insufficiency (OR 4.02), and non-paroxysmal AF (OR 1.90) remain important competing determinants of DRT [4].
- Fourth, any strategy to intensify antithrombotic therapy must be balanced against bleeding, which is not a marginal issue in this population: in a 1,649-patient multicentre study, early nonprocedural bleeding occurred in 7.3% of patients within 3 months, major bleeding in 4.2%, and DAPT at discharge independently increased bleeding risk (aHR 1.61) [9].
Conversely, the small randomised ADALA trial (n=90) suggested that a more tailored strategy may be feasible, with low-dose apixaban reducing the 3-month primary endpoint versus DAPT (4.5% vs 21.7%), with 0% versus 8.7% DRT and numerically fewer major bleeds (4.6% vs 13.0%) [10].
Finally, DRT is not always a one-time event: in a registry of 237 DRT cases, 35.0% showed persistent or recurrent DRT, and this unfavourable evolution doubled thromboembolic risk compared with resolved DRT (26.7% vs 15.1%; HR 2.13) [8].
Therefore, the most defensible clinical interpretation is that this study should refine procedural technique today rather than redefine post-LAAC management tomorrow: optimise implant depth during the index procedure, maintain a lower threshold for CT or TEE surveillance in patients with deep implants or multiple clinical risk factors, and consider antithrombotic intensification only in a selective, bleeding-informed manner.
Current expert consensus and guidelines already support structured imaging follow-up and anticoagulation-based management when DRT is identified, but prospective validation is still needed before CFD-derived scores can be used to de-escalate imaging or individualise therapy in everyday practice [11,12].
References
- Cepas-Guillén P, Albors C, Mill J, Aminian A, Garot P, De Backer O, et al. Impact of device implantation depth on blood flow dynamics after left atrial appendage closure. EuroIntervention. 2026;22:e444-e454. doi:10.4244/EIJ-D-25-01328.
- Zhang S, Xiong S, Guan Y, Zhao X, Qin Y, Guo Z, et al. An updated meta-analysis of device related thrombus following left atrial appendage closure in patients with atrial fibrillation. Front Cardiovasc Med. 2022;9:1088782. doi:10.3389/fcvm.2022.1088782.
- Fauchier L, Cinaud A, Brigadeau F, Lepillier A, Pierre B, Abbey S, et al. Device-Related Thrombosis After Percutaneous Left Atrial Appendage Occlusion for Atrial Fibrillation. J Am Coll Cardiol. 2018;71(14):1528-1536. doi:10.1016/j.jacc.2018.01.076.
- Simard T, Jung RG, Lehenbauer K, Piayda K, Pracoń R, Jackson GG, et al. Predictors of Device-Related Thrombus Following Percutaneous Left Atrial Appendage Occlusion. J Am Coll Cardiol. 2021;78(4):297-313. doi:10.1016/j.jacc.2021.04.098.
- Freixa X, Cepas-Guillen P, Flores-Umanzor E, Regueiro A, Sanchis L, Fernandez-Valledor A, et al. Pulmonary ridge coverage and device-related thrombosis after left atrial appendage occlusion. EuroIntervention. 2021;16(15):e1288-e1294. doi:10.4244/EIJ-D-20-00886.
- Cepas-Guillén P, Flores-Umanzor E, Leduc N, Bajoras V, Perrin N, Farjat-Pasos J, et al. Impact of Device Implant Depth After Left Atrial Appendage Occlusion. JACC Cardiovasc Interv. 2023;16(17):2139-2149. doi:10.1016/j.jcin.2023.05.045.
- Vogl BJ, Vitale E, Ahn S, Sularz A, Chavez Ponce A, Lo Russo GV, et al. Flow Dynamic Factors Correlated With Device-Related Thrombosis After Left Atrial Appendage Occlusion. JACC Adv. 2024;3(11):101339. doi:10.1016/j.jacadv.2024.101339.
- Mesnier J, Simard T, Jung RG, Lehenbauer KR, Piayda K, Pracon R, et al. Persistent and Recurrent Device-Related Thrombus After Left Atrial Appendage Closure: Incidence, Predictors, and Outcomes. JACC Cardiovasc Interv. 2023;16(22):2722-2732. doi:10.1016/j.jcin.2023.09.017.
- Mesnier J, Cruz-González I, Guedeney P, Arzamendi D, Freixa X, Nombela-Franco L, et al. Early Nonprocedural Bleeding After Left Atrial Appendage Occlusion. JACC Cardiovasc Interv. 2024;17(15):1765-1776. doi:10.1016/j.jcin.2024.05.032.
- Freixa X, Cruz-González I, Cepas-Guillén P, et al. Low-Dose Direct Oral Anticoagulation vs Dual Antiplatelet Therapy After Left Atrial Appendage Occlusion: The ADALA Randomized Clinical Trial. JAMA Cardiol. 2024;9(10):922-926. doi:10.1001/jamacardio.2024.2335.
- Saw J, Holmes DR Jr, Cavalcante JL, et al. SCAI/HRS expert consensus statement on transcatheter left atrial appendage closure. J Soc Cardiovasc Angiogr Interv. 2023;2(3):100577. doi:10.1016/j.jscai.2022.100577.
- Goldsweig AM, Glikson M, Joza J, Kavinsky CJ, Khalique O, Lakkireddy D, et al. 2025 SCAI/HRS clinical practice guidelines on transcatheter left atrial appendage occlusion. Heart Rhythm. 2025;22(10):e1048-e1063. doi:10.1016/j.hrthm.2025.05.048.
No comments yet!