02 Jul 2026
Which AF patients may benefit from LAA closure?
Patient selection in 2026
Martin Bergmann reviews the evolving evidence for LAAC, examining how recent landmark trials such as OPTION, CLOSURE‑AF and CHAMPION‑AF are reshaping patient selection and expanding the role of LAAC across a broader spectrum of patients with atrial fibrillation.

Background
Since its introduction to the interventional landscape in 2005, stroke prevention by left atrial appendage closure (LAAC) has been utilised as a treatment option for patients with atrial fibrillation (AF), a CHA2DS2-VASc ≥ 2 and ineligible for long-term oral anticoagulation. The standard patient eligible for LAAC has had bleeding events while on oral anticoagulation LAAC. PRAGUE-17 (n=402, mean CHA2DS2-VASc 4.7) was the first study on an all-comers population and a lower bleeding risk (HAS-BLED ≥2), demonstrating non-inferiority of LAAC vs. DOAC with a 4-year follow-up with a combined primary endpoint for stroke and bleeding events.1
Three large, multicentre trials published in 2025/2026 have evaluated patients w/o increased bleeding risk regarding efficacy and safety of LAAC. These studies impact the shared-decision process with the individual AF patient regarding stroke prevention. While these studies are summarized more extensively elsewhere in this series, the key results relevant for LAAC indication are summarized below.
- OPTION: Patients with atrial fibrillation scheduled for pulmonary vein isolation and a CHA2DS2-VASc ≥2 (men) or ≥3 (women) were eligible to be randomised to anticoagulation with DOAC vs. LAAC employing the WATCHMAN FLX device. LAAC was performed either concomitantly (n=654) or sequentially (n=946, between 90 and 180 days following PVI). The trial proved LAAC in this patient cohort (mean CHA2DS2-VASc 3.5) to be non-inferior to DOAC therapy regarding stroke prevention with fewer clinically relevant bleeding events in the LAAC group at 3 years, although patients were at low risk for bleeding.2
- CLOSURE-AF: This investigator-initiated trial included n=888 patients with a high risk of bleeding events (HAS-BLED 3.0). Mostly elderly patients with a mean CHA2DS2-VASc of 5.2 were randomised to standard care vs. LAAC followed by antiplatelet therapy. The trial did not reach its primary endpoint of non-inferiority for LAAC vs. DOAC therapy. While the number of strokes was identical (n=27/100 patient years in both groups), cardiovascular/unexplained death and major bleeding events were more common > 1 year after the procedure in the LAAC + antiplatelet group.3
- CHAMPION-AF: 3,000 patients indicated for stroke prevention due to elevated CHA2DS2-VASc (mean: 3.5) were randomised to LAAC with the WATCHMAN FLX device vs. DOAC therapy. At three years, statistical non-inferiority was achieved regarding efficacy with very few ischaemic stroke events in both groups (2% and 3.2% DOAC vs. LAAC, respectively). Patients with LAAC experienced fewer clinically relevant bleeding events. 4
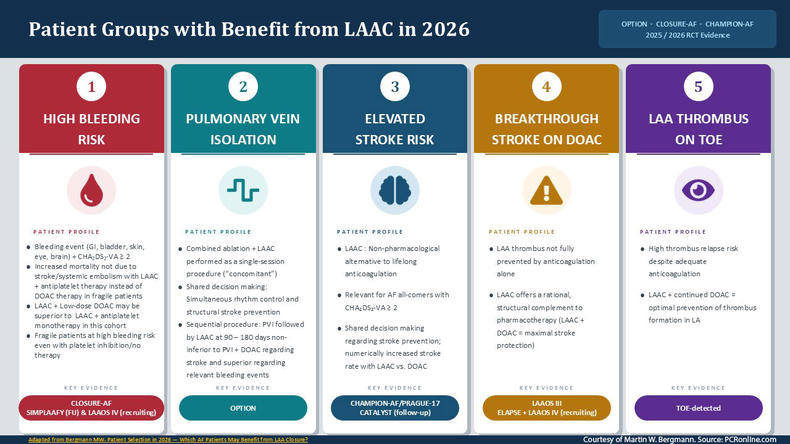
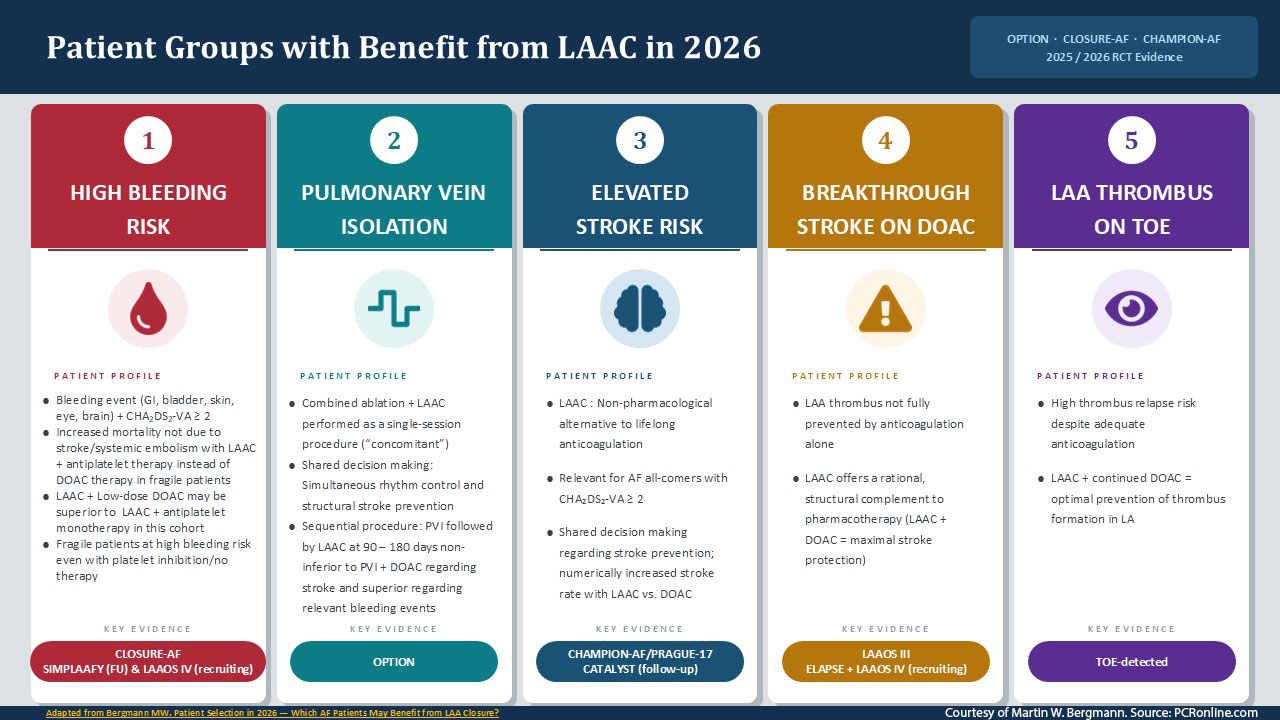
Patient groups which benefit from LAAC in 2026
All trials mentioned above uniformly found the periprocedural risks of LAAC to be low and comparable to AF ablation. Low rates of peri-device leakage (< 2%) and device-related thrombus (around 4%) were observed during follow-up. With improved procedural safety, the landscape for LAAC patient eligibility can be summarized as follows:
- AF patients with high bleeding risk: All three trials proved LAAC to be effective regarding stroke prevention in AF patients. Yet the high-risk and fragile patient group studied in CLOSURE-AF showed high rates of bleeding events despite the absence of DOAC therapy in the LAAC group. This was associated with a higher rate of unexplained/CV death. Post-procedural drug therapy has therefore come into focus for this patient cohort; the combination of low-dose DOAC therapy instead of platelet inhibition, combined with LAAC, may be the best option in this patient cohort. The results of SIMPLAAFY and LAAOS-IV will add to the evidence for this approach; these studies are described in more detail elsewhere in this series.
- AF patients scheduled for pulmonary vein isolation: In a shared decision-making approach, patients may prefer an interventional approach for both rhythm control and stroke prevention. The OPTION trial proves this approach to be safe and feasible; further studies are under way to add more data to this growing field. To achieve optimal results, LAAC planning regarding device sizing is a key component as transient oedema of the pulmonary ridge may affect intra-procedural device sizing. Reimbursement also needs to be addressed: as of June 2026, in Europe only Switzerland has approved concomitant procedures with both devices covered following the FDA’s decision in 2025. Recently, the OPTION-EMEA trial and COCONUT-II trial have been launched to study concomitant PVI + LAAC employing modern EP approaches, namely pulse field ablation.
In the light of growing AF disease burden, interventional LAAC operators should be trained for i.e. PVI by pulse field ablation, resulting in efficient local workflows where EP capacity can be used for more complex procedures where electrophysiological mapping is required (AF redos, flutter, VT, SVT). In concomitant procedures, operators will aim to avoid both complex PVI with anatomic variants of the pulmonary veins as well as complex LAAC; these patients may be more suitable for sequential PVI and LAAC as studies also in OPTION. Cardiac CT will play an important role in identifying such patients. For LAAC, the recently published ELAAC classification system will be helpful to identify complex LAAC anatomies upfront.5 - Concomitant structural procedures in AF patients: Recent smaller series have studied combined procedures like TAVR + LAAC and M-TEER + LAAC. Evidence is still limited but technical feasibility has been demonstrated. More precisely, the WATCH-TAVR study randomized 349 patients to standard medical therapy following TAVR and TAVR/LAAC as a combined procedure finding non-inferiority for clinical endpoints in this series.6
- AF patients with increased stroke risk eligible for DOAC therapy: In a shared decision-making approach, all-comers AF patients may opt for a non-pharmacological approach for stroke prevention. While CHAMPION-AF is the first large trial in this patient group showing non-inferiority, some open questions remain. The results of the CATALYST trial employing the AMULET device for LAAC in an all-comers population will add more evidence. The study landscape regarding these all-comers populations is summarized elsewhere in this series.
- AF patients with a stroke under DOAC therapy: The patient cohort with an ischemic, cardioembolic stroke despite adequate anticoagulation (“breakthrough stroke”) is an increasing clinical observation in many centers with regular neuro-/cardio-board meetings. LAA thrombus formation is not completely prevented by DOAC therapy; LAAC plus continued full-dose DOAC therapy is a rational treatment option in this patient cohort. The currently recruiting ELAPSE trial will add evidence to this approach.
- AF patients with LAA thrombus: LAA thrombus is regularly detected in patients scheduled for cardioversion receiving a TOE. These thrombi regularly disappear with anticoagulation over four weeks, yet there is a high risk of relapse even if the patients remain on DOAC´s. Therefore, LAAC needs to be discussed in this patient cohort; importantly, these patients also have an increased risk of device-related thrombi and need to remain on oral anticoagulation.
References
- Osmancik P, Herman D, Neuzil P, et al. 4-Year Outcomes After Left Atrial Appendage Closure Versus Nonwarfarin Oral Anticoagulation for Atrial Fibrillation. J Am Coll Cardiol 2022;79:1-14. doi: 10.1016/j.jacc.2021.10.023
- Wazni OM, Saliba WI, Nair DG, et al. Left Atrial Appendage Closure after Ablation for Atrial Fibrillation. N Engl J Med 2025;392:1277-1287. doi: 10.1056/NEJMoa2408308
- Landmesser U, Skurk C, Kirchhof P, et al. Left Atrial Appendage Closure or Medical Therapy in Atrial Fibrillation. N Engl J Med 2026;394:1270-1280. doi: 10.1056/NEJMoa2513310
- Doshi SK, Kar S, Nair DG, et al. Left Atrial Appendage Closure or Anticoagulation for Atrial Fibrillation. N Engl J Med 2026;394:2083-2094. doi: 10.1056/NEJMoa2517213
- Nielsen-Kudsk JE, Aminian A, Backer O, et al. A new implanter classification system for left atrial appendage closure from the European Left Atrial Appendage Closure Club (ELAACC). EuroIntervention 2025;21:e594-e604. doi: 10.4244/EIJ-D-24-00954
- Kapadia SR, Krishnaswamy A, Whisenant B, et al. Concomitant Left Atrial Appendage Occlusion and Transcatheter Aortic Valve Replacement Among Patients With Atrial Fibrillation. Circulation 2024;149:734-743. doi: 10.1161/CIRCULATIONAHA.123.067312
