21 Mar 2026
Redo TAVI: essential considerations for lifetime valve management
In this article, Ahmed Abdelhafez and Mohamed Abdel-Wahab review the key principles of redo TAVI, a procedure set to become increasingly common as TAVI expands to younger and lower-risk patients. They discuss the major challenges of coronary obstruction, device selection, and implantation strategy, highlighting how careful planning at the index procedure is critical to ensuring safe and effective future valve interventions.

Essentials to know for Redo TAVI
Transcatheter aortic valve implantation (TAVI) is increasingly performed in younger, lower-risk patients who will outlive their first transcatheter heart valve (THV), so redo TAVI is set to become a common reintervention rather than a rare salvage procedure1,2.
Modelling of United States and Japanese registry data projects that redo TAVI will overtake TAVI-in-surgical-valve to dominate the valve-in-valve market within the next decade, approaching 15% of all US TAVI procedures by 20353. Early multicentre evidence is reassuring; in the prospective ReTAVI registry of 143 patients treated with a balloon-expandable SAPIEN 3 (Edwards Lifesciences), the second valve was implanted successfully in 95.1%, with 3.5% 30-day mortality and a mean gradient reduction of 12 mmHg overall1. Good outcomes, however, depend heavily on anatomy and planning. Three questions dominate.
Risk of coronary obstruction
When the second THV pins the index leaflets open, it creates a covered cylinder — a “neoskirt” — that can cover a coronary ostium directly or seal the sinus of Valsalva against the sinotubular junction (STJ), causing sinus sequestration4,5. This is the defining hazard of redo TAVI and is far more relevant than in an index procedure. Computed tomography (CT)-based studies predict that redo TAVI would be unfeasible or carry high coronary risk in a significant proportion of patients, particularly with tall-frame supra-annular index valves, whose high leaflets produce a taller neoskirt4,6. Risk increases with a narrow STJ and with index leaflets extending above the STJ4.
Reassuringly, in the ReTAVI registry, clinical coronary obstruction occurred in only 1.4%1. Systematic CT assessment and risk assessment algorithms, facilitated by dedicated planning tools such as the Redo-TAV app, define candidacy, with a valve-to-aorta distance <2 mm marking high risk5,7. In cases at risk of coronary obstruction, coronary protection, primarily by leaflet modification techniques, is planned in advance8. However, its efficacy is limited when the commissural posts or internal skirt of the second valve cause coronary obstruction by sinus sequestration9.
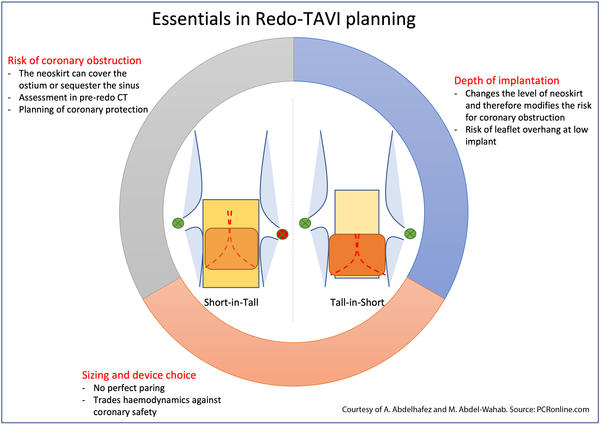
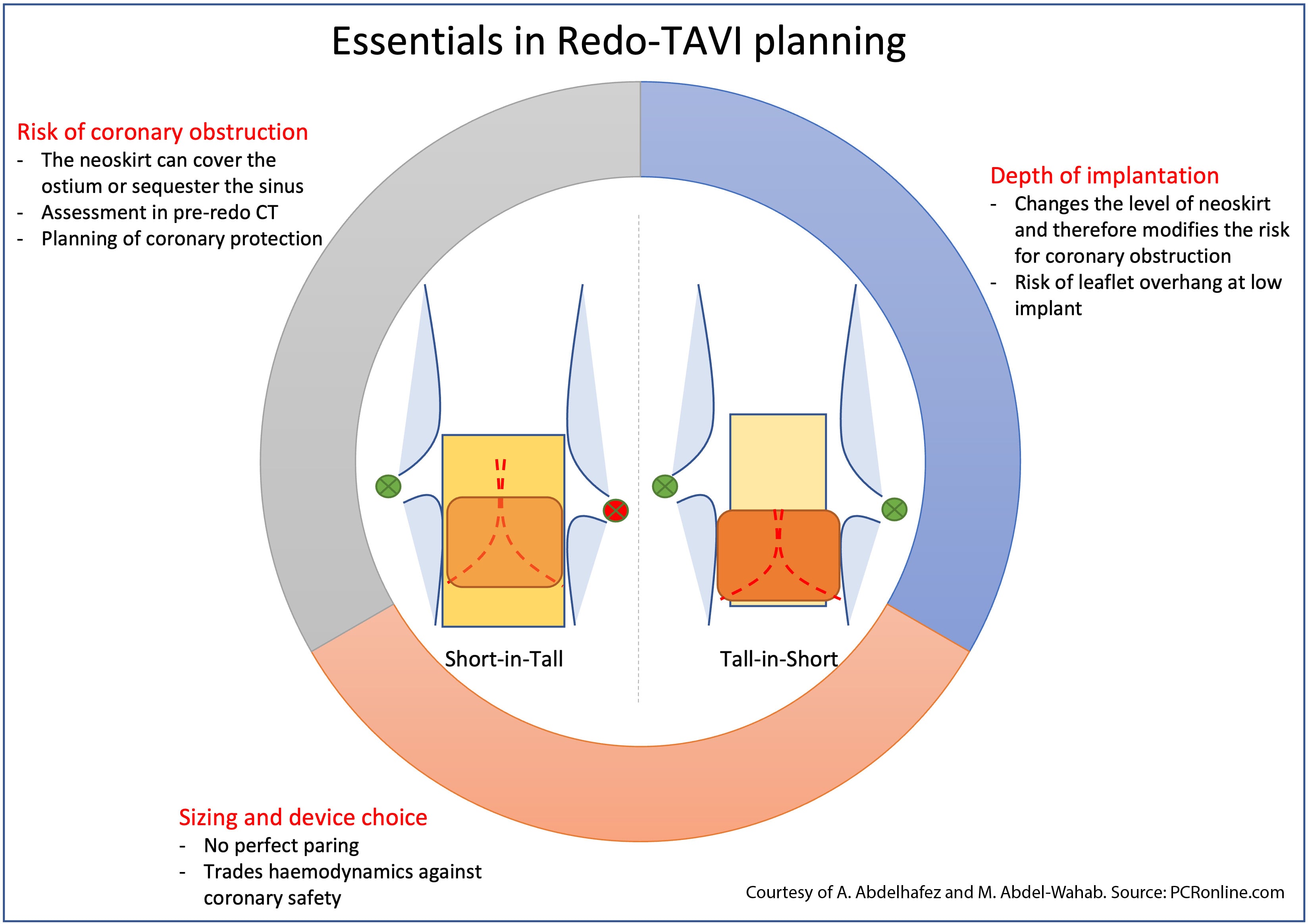
Sizing and device choice
There is no universal best combination (figure 1); each pairing trades haemodynamics against coronary safety. A short-frame valve inside a tall-frame one (short-in-tall) yields an adjustable neoskirt and a more favourable coronary access profile depending on implant depth, whereas a tall-frame second valve (e.g. tall-in-short) tends to give lower gradients but a taller neoskirt5,10. The index frame dictates the redo plan: a balloon-expandable valve may further expand a self-expanding frame, especially if it was underexpanded; therefore, native annular sizing and preferably pre-index TAVI CT should be considered when planning a redo TAVI5. The small annulus is the most difficult scenario, where limited internal dimensions compound patient–prosthesis mismatch and narrow the safe redo options — an argument, at the index procedure, for choosing a valve that preserves future reintervention, subscribing to a lifetime management strategy.
Depth of implantation of the second THV
For any given combination, implant depth is the most powerful modifiable determinant of coronary risk. A lower second-THV implant lowers the functional neoskirt and can convert an unfavourable anatomy into a feasible one. In a CT analysis, a low SAPIEN 3 position rendered redo TAVI feasible in over 98% of cases, irrespective of index implant depth11. The trade-off is greater leaflet overhang, which on the bench does not appear to compromise hydrodynamic performance but remains unproven in heavily degenerated, calcified valves10. Conversely, despite the use of leaflet modification, higher implantation in small anatomies may itself risk sinus sequestration: the inner skirt — or a misaligned commissural post — of the second valve can obstruct the lacerated leaflet splay even after successful leaflet modification9.
Key messages
- Lifetime management begins at the first TAVI. Index valve type and implant height set the relationship between coronary height and neoskirt extension, while commissural alignment of the index valve is decisive for the feasibility of later leaflet modification — together these determine whether a redo-TAVI is straightforward, high-risk, or unfeasible. Optimising the index procedure is the single most effective way to ensure an uncomplicated redo.
- Coronary obstruction is the defining risk of redo-TAVI and is substantially more relevant than for index TAVI; systematic CT screening, with coronary protection when indicated, is mandatory. Observed rates are low in well-selected cohorts (0.9-1.4%).
- Implant depth and device choice are the key procedural levers: a lower second-valve implant and a shorter redo frame both reduce neoskirt height and preserve coronary access
References
- Tarantini G, Nai Fovino L, Alvarez Covarrubias H, Wolny R, Fabris T, Nawara-Skipirzepa J, et al. Early outcomes of redo-TAVI with the SAPIEN 3 platform: the prospective, multicentre ReTAVI registry. EuroIntervention. 2026 Jun;22(11).
- Landes U, Webb JG, De Backer O, Sondergaard L, Abdel-Wahab M, Crusius L, et al. Repeat transcatheter aortic valve replacement for transcatheter prosthesis dysfunction. J Am Coll Cardiol. 2020 Apr;75(16):1882–1893.
- Ohno Y, Généreux P, Dar RD, Gerckens U, Dvir D, Tchétché D, et al. Predicting the surge in valve-in-valve volume: a comparative study of Japan and the United States. JACC Asia. 2025 Oct;5(10):1288–1297.
- Ochiai T, Oakley L, Sekhon N, Komatsu I, Flint N, Kaewkes D, et al. Risk of coronary obstruction due to sinus sequestration in redo transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2020 Nov;13(22):2617–2627.
- Bapat VN, Fukui M, Zaid S, Okada A, Jilaihawi H, Rogers T, et al. A guide to transcatheter aortic valve design and systematic planning for a redo-TAV (TAV-in-TAV) procedure. JACC Cardiovasc Interv. 2024 Jul;17(14):1631–1651.
- Meier D, Akodad M, Landes U, Barlow AM, Chatfield AG, Lai A, et al. Coronary access following redo TAVR: impact of THV design, implant technique, and cell misalignment. JACC Cardiovasc Interv. 2022 Aug;15(15):1519–1531.
- Abdelhafez A, Lankisch N, Iannopollo G, Dumpies O, Rotta detto Loria J, Richter I, et al. CT-based risk stratification of coronary obstruction during TAVR: clinical utility and a new volumetric parameter. JACC Cardiovasc Interv. 2026 Jun;19(11):1406–1419.
- Khan JM, Greenbaum AB, Babaliaros VC, Rogers T, Eng MH, Paone G, et al. The BASILICA trial: prospective multicenter investigation of intentional leaflet laceration to prevent TAVR coronary obstruction. JACC Cardiovasc Interv. 2019 Jul;12(13):1240–1252.
- Abdelhafez A, Khokhar AA, Beneduce A, de Backer O, Abdel-Wahab M. Commissural misalignment–mediated sinus sequestration following balloon-augmented BASILICA during redo-TAVR. JACC Cardiovasc Interv. 2026 Jun;19(11):1516–1519.
- Akodad M, Sellers S, Landes U, Meier D, Tang GHL, Gada H, et al. Balloon-expandable valve for treatment of Evolut valve failure: implications on neoskirt height and leaflet overhang. JACC Cardiovasc Interv. 2022 Feb;15(4):368–377.
- Kobari Y, Khokhar AA, Lulic D, Kofoed KF, Fuchs A, Bieliauskas G, et al. Impact of transcatheter aortic valve design and implant strategy on redo-TAVR feasibility: a CT-based analysis. JACC Cardiovasc Interv. 2025 May;18(9):1206–1208.
Authors

