18 Jun 2026
When transfemoral TAVI is not an option: rethinking alternative access strategies
In this article, Ulrich Schäfer explores the evolving landscape of access strategies in transcatheter aortic valve implantation (TAVI). While the transfemoral approach remains the gold standard, a significant proportion of patients are not suitable due to peripheral vascular disease or anatomical constraints.
Drawing on clinical evidence and real-world practice, learn about the range of alternative access routes now available, from transaxillary and transcarotid to transcaval and direct aortic approaches, and their respective advantages, limitations, and outcomes.

Over the last two decades, transcatheter aortic valve implantation (TAVI) has emerged as a valuable treatment option (Class I, Level B) for patients with severe aortic stenosis (AS) who are at higher or moderate surgical risk for conventional aortic valve replacement with an age of ≥ 70 years.1 Nowadays, the most frequently used access route utilizes the common femoral artery. But whenever the transfemoral (TF) approach for TAVI or a surgical aortic valve replacement is not feasible, an alternative access route has to be considered (Class IIa LoE C).1
In recent years, the transapical (TA) approach has been largely displaced by other transvascular access routes, due to accumulating evidence that the TA approach is more likely associated with a higher morbidity compared to transvascular access routes.2 In this regard, a recent study comprising 129,821 patients of the national inpatient database (NID) of the United States (years 2011 to 2017) described the rapid decrease of TA utilization. After peaking numbers in 2013 at 27.7%, the counts declined to 1.92% in 2017, which was accompanied by a higher inpatient mortality, increased length of stay, and higher costs in those patients with TA-TAVI.3
Nevertheless, peripheral vascular disease is a common finding in patients who are candidates for TAVI.4 For transvascular TAVI sheath/introducer sizes range between 14F and 20F, depending on the valve size and the transcatheter heart valve (THV) delivery system. Thus, for most devices, a minimal vessel diameter of 5 to 6 mm is required. In addition, in at least 10 to 15% of TAVI patients, a transfemoral (TF) approach seems to be not advisable due to significant peripheral artery disease or severe vessel tortuosity. Hence, the direct aortic (Tao), transcarotid (TC), transcaval (TCav), and transaxillar (TAX) implantation routes have been developed and applied to a broader extent over the last decade, but these alternative access routes are still more frequently utilized in experienced high-volume centers.5-9
According to BiBa MedTech Research, the counts demonstrated a continuous rise between 2013 and 2025 for TF access utilization (in 2025: Europe 96%, Germany 94%; see figure 1). Conversely, the largest decrease was found for the TA access route (in 2025: Europe 1%, Germany 3%) with similarly stable counts for the TAX access route (in 2025: Europe 2%, Germany 1%), TC/TCav access route (in 2025: Europe 1%, Germany 1%), whereas the TAO access route seems no longer to be utilized in Europe and Germany, respectively.
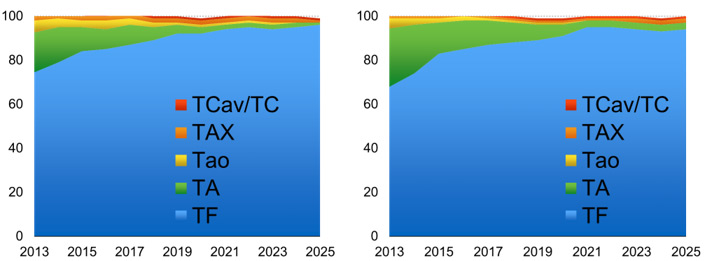
Figure 1
Until today, there is a great amount of variability in access utilization among various centers with regard to their first and second choice of access for TAVI. In some hospitals, the TAX approach is used in up to 20% of the cases.10 Unfortunately, alternative TAVI approaches have not been studied in a comparative fashion, but available data suggest better outcomes for transvascular techniques compared to TA-TAVI (table 1). But the choice of alternative access routes depends still mainly on the experience and judgment of the heart team. Nevertheless, judgment of invasiveness varies among different investigators. Nevertheless, "central" access routes (e.g. TA and Tao) are associated with an even small thoracotomy, mandating intubation and ventilation, whereas other "peripheral" transvascular approaches allow for analgosedation and/or local anesthesia, only (figure 2).
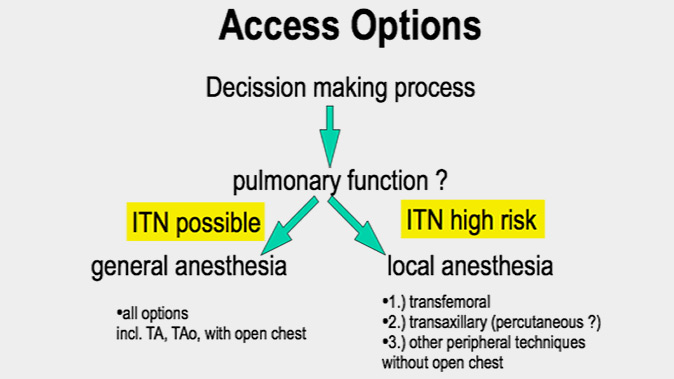
Figure 2
The various levels of invasiveness with corresponding outcomes vary between different access approaches and are derived from the available literature (table 1).
Table 1
Apical | Aortic | Axillar | Axillar (perc.) | Carotid | Caval | |
|---|---|---|---|---|---|---|
Thourani 2015 | Babat 2016 | Petronio 2012 | Schäfer 2010, 2016 | Mylotte 2016 | Greenbaum 2016 | |
N | 4085 | 301 | 141 | 100 | 96 | 100 |
Centers | Many | 18 | 10 | 2 | 3 | 17 |
STS | 8.8 (5.8,13) | 9.0 ± 7.6 | no data | 7.2±5.2 | 7.1 ± 4.2 | 9.6 ± 6.3 |
LOS - days | 8.9 ± 6.4 | 9.9 ± 8.5 | no data | 7.9 ± 9.4 | 11 (9, 15) | 4 (2, 6) |
AKIN | 38.8% | 9.5% | 4.3% | 3 % | 7.3% | 3% |
LT Bleeding | no data | 3.4% | 7.8% | 0 % | 4.2% | 7% |
Vascular comp (maj.) | <1% | 3.4% | 2.2% | 1 % | 4.2% | 12% |
30-d Stroke/TIA | 2.4% | 1.3% | 2.1% | 1 % | 6.3% | 5% |
30-day Mortality | 8.8% | 6.1% | 5.7% | 6 % | 6.3% | 8% |
Notes | Self-reported | >5 cases prior to enrollment | Self-reported | Self-reported | No systematic imaging | Adjudicated / Systematic CT |
Moreover, practicability, ergonomics and costs differ between various access approaches, which have been presented at several scientific meetings and represent to some extent the opinion of the author (table 2).
Table 2
Apical | Aortic | Axillar | Carotid | Caval | |
|---|---|---|---|---|---|
Pain | Poor | Poor | Good | Good | Good |
Bleeding | Poor | Fair | Good | Good | Poor |
LOS | Poor | Poor | Good | Good | Fair |
Outcomes | Poor | Good | Good | Good | Fair |
Supportive Evidence | Good | Good | Good | Poor | Fair |
TAVI Ergonomics | Poor | Poor | Fair | Poor | Fair |
Procedure Complexity | Good | Fair | Fair | Fair | Poor |
Costs | Low | Low | Low | Low | Fair |
In summary
The frequencies of alternative access routes have been significantly declining in recent years, but they still serve as an important supplement for those patients in whom the TF access route is not advisable. Each alternative access has advantages and disadvantages, so the access route should be tailored to the patient's characteristics. However, there is no standardized algorithm for choosing the optimal alternative vascular access. In addition, the TA access seems to be limited to a very selected subset of patients with no other options. Possibly, TA-TAVI will be completely eliminated in the near future, since the industry is no longer pursuing sales in a significantly declining market.
References
- Praz F, Borger MA, Lanz J, Marin-Cuartas M, Abreu A, Adamo M, Marsan NA, Barili F, Bonaros N, Cosyns B, De Paulis R, Gamra H, Jahangiri M, Jeppsson A, Klautz R, Mores B, Pérez-David E, Pöss J, Prendergast BD, Rocca B, Rossello X, Suzuki M, Thiele H, Tribouilloy CM, Wojakowski W. ESC/EACTS Scientific Document Group , 2025 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), European Heart Journal, 2025; Volume 46, Issue 44: 4635–4736.
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Lenard Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BP, Sádaba JR, Tribouilloy C, Wojakowski W. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022 Feb 12;43(7):561-632.
- Sohal S, Mehta H, Kurpad K, Mathai SV, Tayal R, Visveswaran GK, Wasty N, Waxman S, Cohen M. Declining Trend of Transapical Access for Transcatheter Aortic Valve Replacement in Patients with Aortic Stenosis. J Interv Cardiol. 2022: 1-6.
- Smith CR, Leon MB, Mack MJ, Miller C, Moses JM, Svensson LG, Tuzcu M, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ, PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med 2011;364:2187-2198.
- Lanz J, Greenbaum A., Pilgrim T., Tarantini G., Windecker S. Current state of alternative access for transcatheter aortic valve implantation. EuroIntervention. 2018; 14 (AB40-AB52. Aug 31).
- Eng MH, Qintar M, Apostolou D, O'Neill WW. Alternative Access for Transcatheter Aortic Valve Replacement: A Comprehensive Review. Interv Cardiol Clin. 2021 Oct;10(4):505-517.
- Morello A, Corcione N, Ferraro P, Cimmino M, Pepe M, Cassese M, Frati G, Biondi-Zoccai G, Giordano A. The best way to transcatheter aortic valve implantation: From standard to new approaches. Int J Cardiol. 2021 Jan 1;322:86-94.
- Banks A, Gaca J, Kiefer T. Review of alternative access in transcatheter aortic valve replacement. Cardiovasc Diagn Ther. 2020 Feb;10(1):72-82.
- Young MN, Singh V, Sakhuja R. A Review of Alternative Access for Transcatheter Aortic Valve Replacement. Curr Treat Options Cardiovasc Med. 2018 Jul 4;20(7):62.
- Petronio AS, De Carlo M, Bedogni F, Maisano F, Ettori F, Klugmann S, Poli A, Marzocchi A, Santoro G, Napodano M, Ussia GP, Giannini C, Brambilla N, Colombo A. 2-year results of CoreValve implantation through the subclavian access: a propensity-matched comparison with the femoral access. Am Coll Cardiol 2012;60:502-507.
- Schäfer U, Ho Y, Frerker C, Schewel D, Sanchez-Quintana D, Schofer J, Bijuklic K, Meincke F, Thielsen T, Kreidel F, Kuck KH. Direct percutaneous access technique for transaxillary transcatheter aortic valve implantation: "the Hamburg Sankt Georg approach". JACC Cardiovasc Interv 2012;5:477-486.
- Schäfer U, Deuschl F, Schofer N, Frerker C, Schmidt T, Kuck KH, Kreidel F, Schirmer J, Mizote I, Reichenspurner H, Blankenberg S, Treede H, Conradi L. Safety and efficacy of the percutaneous transaxillary access for transcatheter aortic valve implantation using various transcatheter heart valves in 100 consecutive patients. Int J Cardiol. 2017 Apr 1;232:247-254.
- Mylotte D, Sudre A, Teiger E, Obadia JF, Lee M, Spence M, Khamis H, Al Nooryani A, Delhaye C, Amr G, Koussa M, Debry N, Piazza N, Modine T. Transcarotid Transcatheter Aortic Valve Replacement: Feasibility and Safety. JACC Cardiovasc Interv. 2016;9(5):472-480.
- Greenbaum AB, O'Neill WW, Paone G, Guerrero ME, Wyman JF, Cooper RL, Lederman RJ. Caval-aortic access to allow transcatheter aortic valve replacement in otherwise ineligible patients: initial human experience. J Am Coll Cardiol. 2014; 63(25 Pt A):2795-2804.
- Greenbaum AB, Babaliaros VC, Chen MY, Stine AM, Rogers T, O'Neill WW, Paone G, Thourani VH, Muhammad KI, Leonardi RA, Ramee S, Troendle JF, Lederman RJ. Transcaval Access and Closure for Transcatheter Aortic Valve Replacement: A Prospective Investigation. J Am Coll Cardiol. 2017;69(5):511-521.
- Bapat V, Frank D, Cocchieri R, Jagielak D, Bonaros N, Aiello M, Lapeze J, Laine M, Chocron S, Muir D, Eichinger W, Thielmann M, Labrousse L, Rein KA, Verhoye JP, Gerosa G, Baumbach H, Bramlage P, Deutsch C, Thoenes M, Romano M. Transcatheter Aortic Valve Replacement Using Transaortic Access: Experience From the Multicenter, Multinational, Prospective ROUTE Registry. JACC Cardiovasc Interv. 2016;9(17):1815-1822.
- Thourani VH, Jensen HA, Babaliaros V, Suri R, Vemulapalli S, Dai D, Brennan JM, Rumsfeld J, Edwards F, Tuzcu EM, Svensson L, Szeto WY, Herrmann H, Kirtane AJ, Kodali S, Cohen DJ, Lerakis S, Devireddy C, Sarin E, Carroll J, Holmes D, Grover FL, Williams M, Maniar H, Shahian D, Mack M. Transapical and Transaortic Transcatheter Aortic Valve Replacement in the United States. Ann Thorac Surg. 2015 Nov;100(5):1718-1726.
Conflict of Interest
U. Schäfer has received honoraria due to advisory board activities and grant support from Abbott Vascular, Medtronic Inc. New Valve Technology, Edwards Lifesciences, as well as honoraria from the speakers bureau of Edwards Lifesciences, Boston Scientific, New Valve Technology, Abbott Vascular, and Medtronic Inc.
